

Schneider membrane elevation in presence of sinus septa: anatomic features and surgical management
- PMID: 22848223
- PMCID: PMC3405661
- DOI: 10.1155/2012/261905
Schneider membrane elevation in presence of sinus septa: anatomic features and surgical management
Abstract
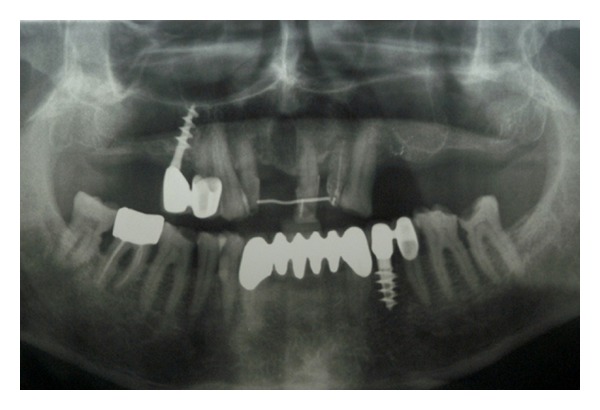
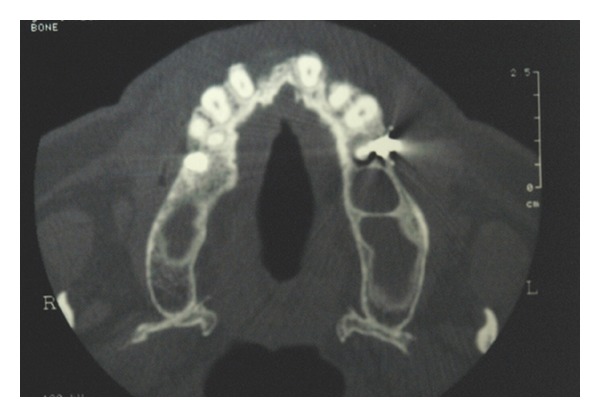
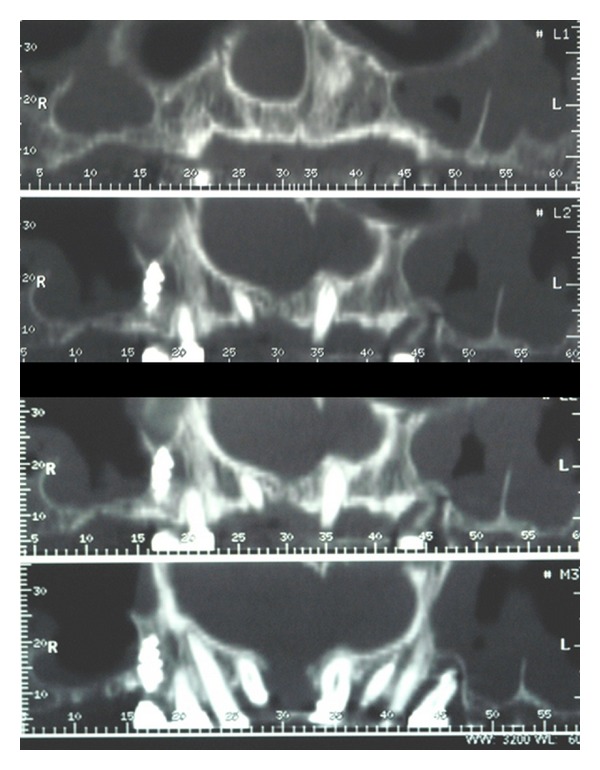
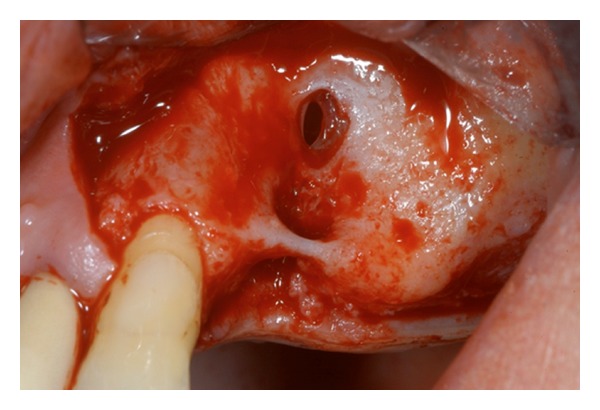
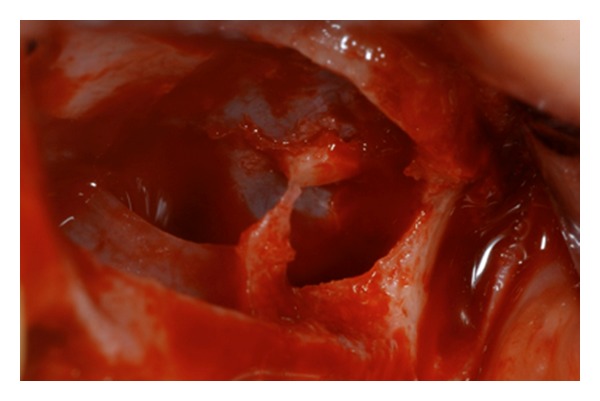
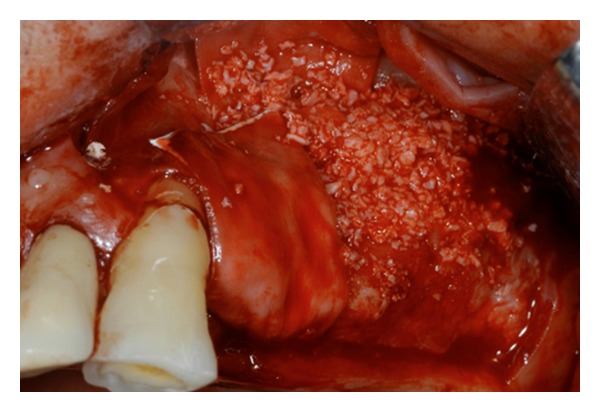
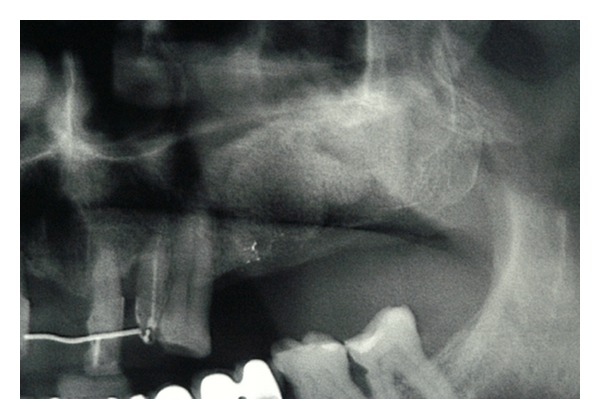
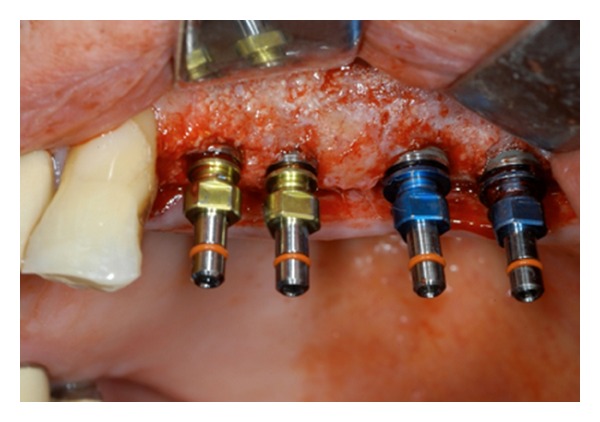
Maxillary sinus floor elevation via a lateral approach is a predictable technique to increase bone volume of the edentulous posterior maxilla and consequently for dental implants placement. The sinus floor is elevated and it can be augmented with either autologous or xenogeneic bone grafts following an opening bone window created on the facial buccal wall. Maxillary septa are walls of cortical bone within the maxillary sinus. The septa shape has been described as an inverted gothic arch arising from the inferior or lateral walls of the sinus and may even divide the sinus into two or more cavities. Some authors have reported a higher prevalence of septa in atrophic edentulous areas than in nonatrophic ones. Radiographic identification of these structures is important in order to perform the right design of the lateral window during sinus lift. Aim of this investigation is to highlight the correct steps for doing sinus lift surgery in presence of those anatomic variations. Clinicians should always perform clinical and radiographic diagnosis in order to avoid complications related to the sinus lift surgery.
Figures


References
-
- Tatum H., Jr. Maxillary and sinus implant reconstructions. Dental Clinics of North America. 1986;30(2):207–229. - PubMed
-
- Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. Journal of Oral Surgery. 1980;38(8):613–616. - PubMed
-
- Vinter I, Krmpotic-Nemanic J, Hat J, Jalsovec D. Does the alveolar process of the maxilla always disappear after loss of teeth? Laryngorhinootologie. 1993;72(12):605–607. - PubMed
-
- Sailer HF. A new method of inserting endosseous implants in totally atrophic maxillae. Journal of Cranio-Maxillo-Facial Surgery. 1989;17(7):299–305. - PubMed
-
- Triplett RG, Nevins M, Marx RE, et al. Pivotal, randomized, parallel evaluation of recombinant human bone morphogenetic protein-2/absorbable collagen sponge and autogenous bone graft for maxillary sinus floor augmentation. Journal of Oral and Maxillofacial Surgery. 2009;67(9):1947–1960. - PubMed
