

Association between endoscopic vs open vein-graft harvesting and mortality, wound complications, and cardiovascular events in patients undergoing CABG surgery
- PMID: 22851114
- PMCID: PMC3699197
- DOI: 10.1001/jama.2012.8363
Association between endoscopic vs open vein-graft harvesting and mortality, wound complications, and cardiovascular events in patients undergoing CABG surgery
Abstract
Context: The safety and durability of endoscopic vein graft harvest in coronary artery bypass graft (CABG) surgery has recently been called into question.
Objective: To compare the long-term outcomes of endoscopic vs open vein-graft harvesting for Medicare patients undergoing CABG surgery in the United States.
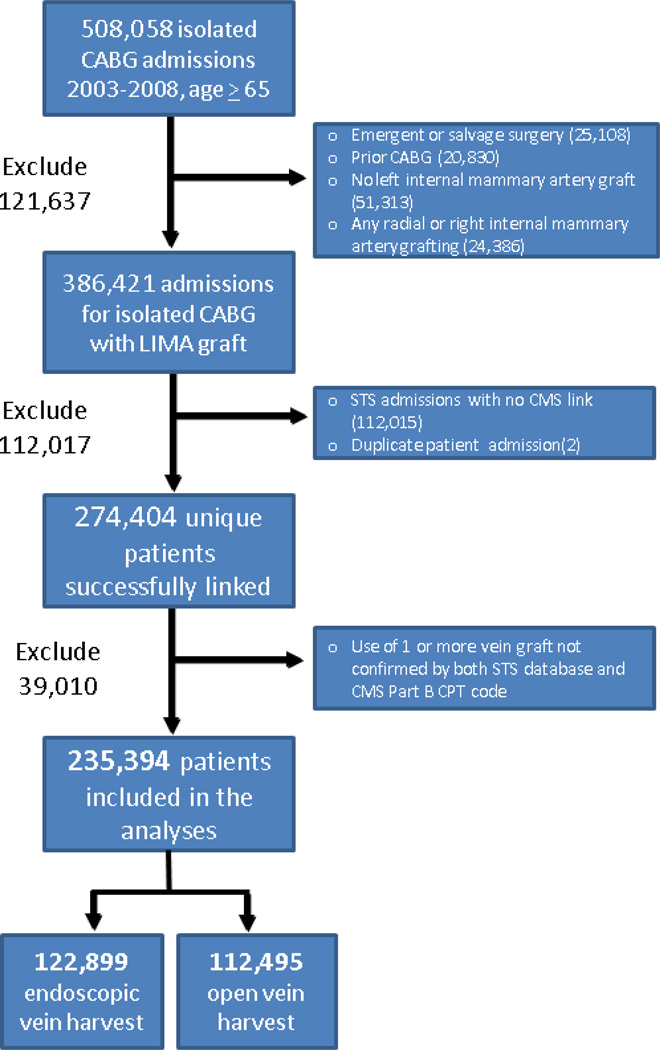
Design, setting, and patients: An observational study of 235,394 Medicare patients undergoing isolated CABG surgery between 2003 and 2008 at 934 surgical centers participating in the Society of Thoracic Surgeons (STS) national database. The STS records were linked to Medicare files to allow longitudinal assessment (median 3-year follow-up) through December 31, 2008.
Main outcome measures: All-cause mortality. Secondary outcome measures included wound complications and the composite of death, myocardial infarction, and revascularization.
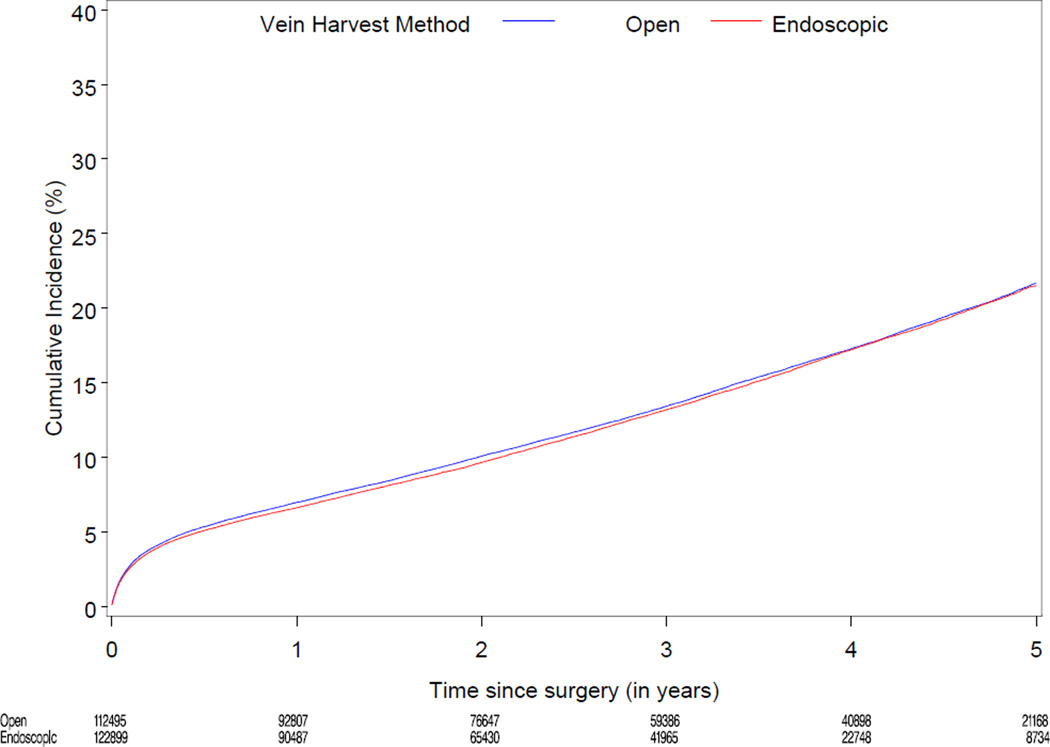
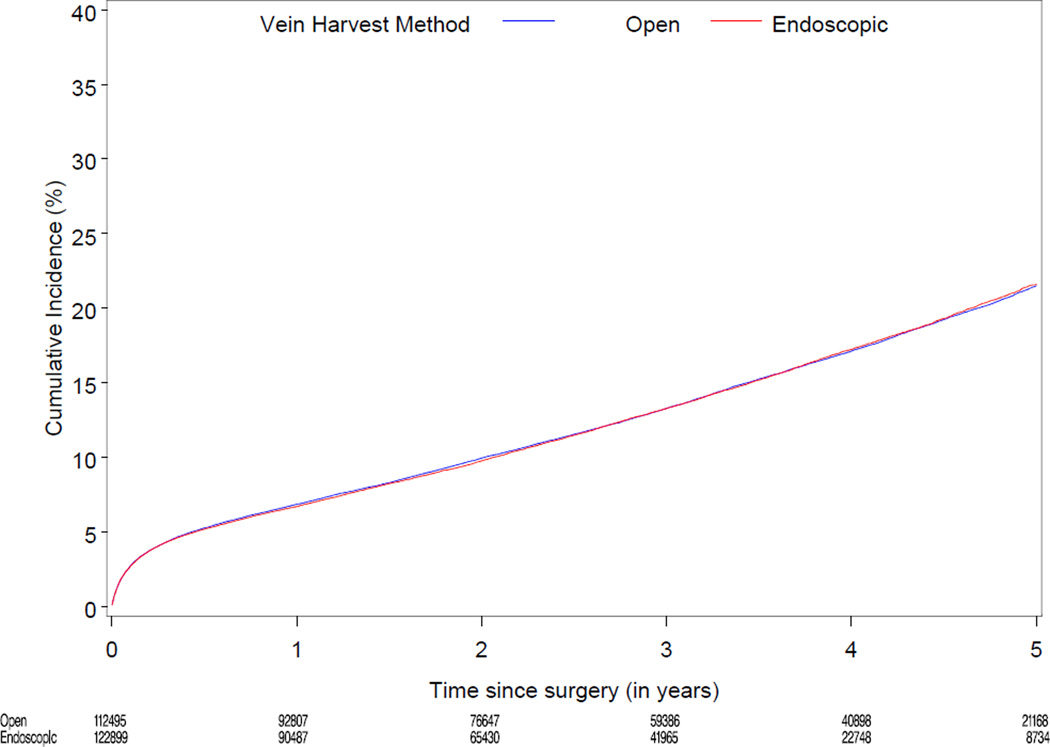
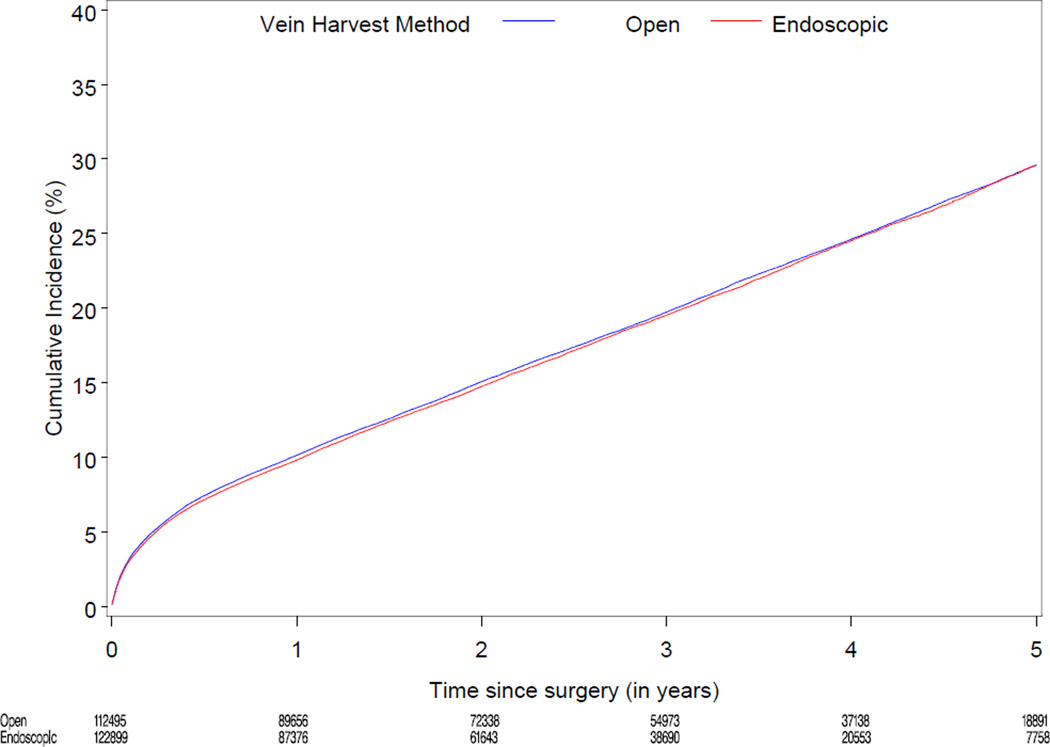
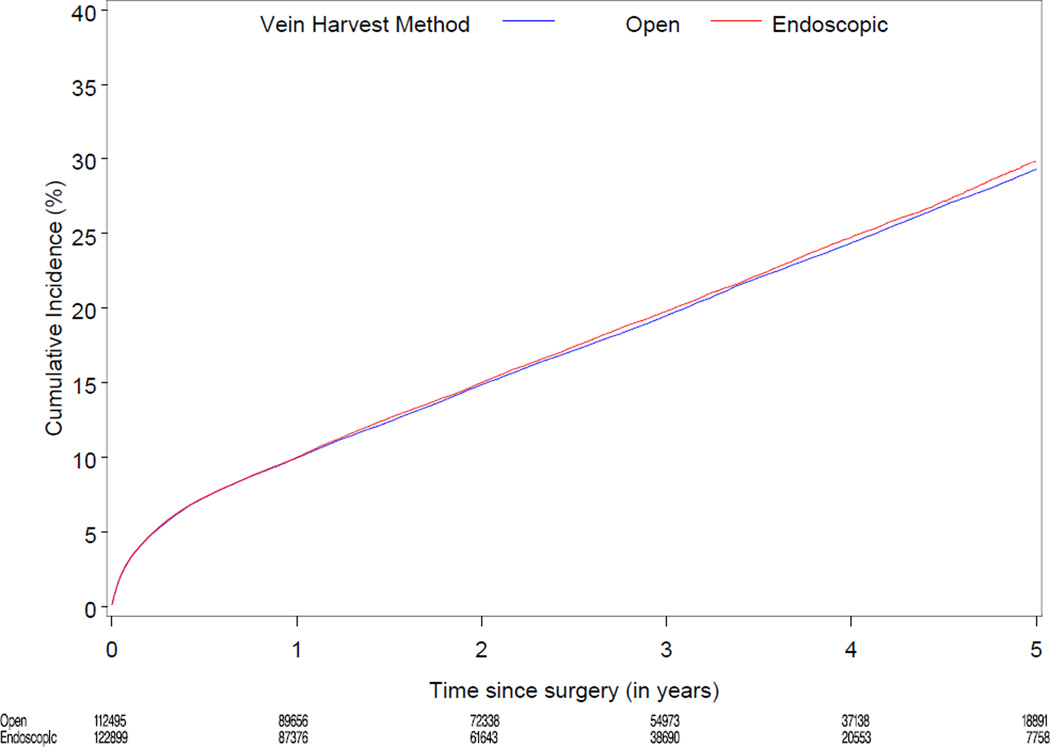
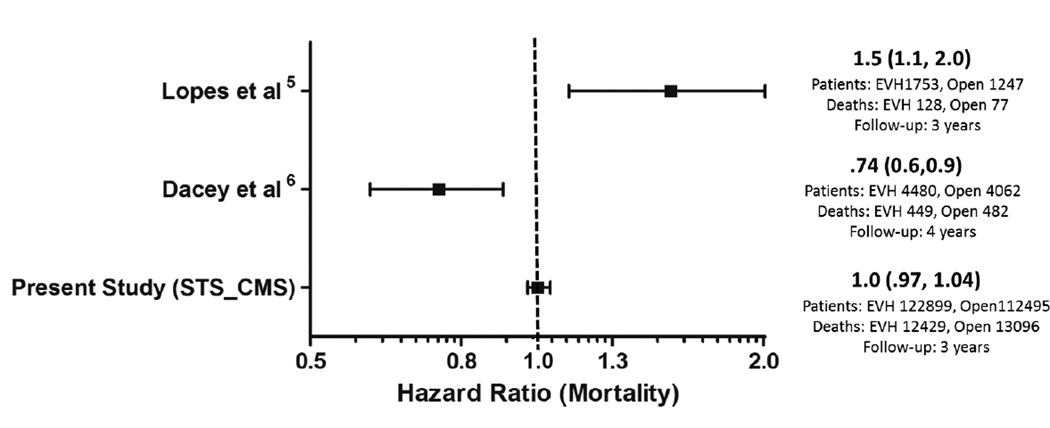
Results: Based on Medicare Part B coding, 52% of patients received endoscopic vein-graft harvesting during CABG surgery. After propensity score adjustment for clinical characteristics, there were no significant differences between long-term mortality rates (13.2% [12,429 events] vs 13.4% [13,096 events]) and the composite of death, myocardial infarction, and revascularization (19.5% [18,419 events] vs 19.7% [19,232 events]). Time-to-event analysis for those patients receiving endoscopic vs open vein-graft harvesting revealed adjusted hazard ratios [HRs] of 1.00 (95% CI, 0.97-1.04) for mortality and 1.00 (95% CI, 0.98-1.05) for the composite outcome. Endoscopic vein-graft harvesting was associated with lower harvest site wound complications relative to open vein-graft harvesting (3.0% [3654/122,899 events] vs 3.6% [4047/112,495 events]; adjusted HR, 0.83; 95% CI, 0.77-0.89; P < .001).
Conclusion: Among patients undergoing CABG surgery, the use of endoscopic vein-graft harvesting compared with open vein-graft harvesting was not associated with increased mortality.
Figures
Comment in
-
Endoscopic vein-graft harvest is safe for CABG surgery.JAMA. 2012 Aug 1;308(5):512-3. doi: 10.1001/jama.2012.9079. JAMA. 2012. PMID: 22851118 No abstract available.
-
Vein-graft harvesting technique in coronary artery bypass graft surgery.JAMA. 2012 Nov 7;308(17):1739; author reply 1739-40. doi: 10.1001/jama.2012.14015. JAMA. 2012. PMID: 23117767 No abstract available.
-
How good is "good enough"?JAMA Surg. 2013 Jan;148(1):10-1. doi: 10.1001/jamasurg.2013.617. JAMA Surg. 2013. PMID: 23324832
References
-
- Lumsden AB, Eaves FF, 3rd, Ofenloch JC, Jordan WD. Subcutaneous, video-assisted saphenous vein harvest: report of the first 30 cases. Cardiovasc Surg. 1996 Dec;4(6):771–776. - PubMed
-
- Allen KB, Griffith GL, Heimansohn DA, et al. Endoscopic versus traditional saphenous vein harvesting: a prospective, randomized trial. Ann Thorac Surg. 1998 Jul;66(1):26–31. discussion 31-22. - PubMed
-
- Puskas JD, Wright CE, Miller PK, et al. A randomized trial of endoscopic versus open saphenous vein harvest in coronary bypass surgery. Ann Thorac Surg. 1999 Oct;68(4):1509–1512. - PubMed
-
- Shahian D, O'Brien SM, Filardo G, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1--coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88(1 Suppl):S2–S22. - PubMed
-
- Lopes RD, Hafley GE, Allen KB, et al. Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery. N Engl J Med. 2009 Jul 16;361(3):235–244. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
