

Randomized trial of radiation therapy plus procarbazine, lomustine, and vincristine chemotherapy for supratentorial adult low-grade glioma: initial results of RTOG 9802
- PMID: 22851558
- PMCID: PMC3732006
- DOI: 10.1200/JCO.2011.35.8598
Randomized trial of radiation therapy plus procarbazine, lomustine, and vincristine chemotherapy for supratentorial adult low-grade glioma: initial results of RTOG 9802
Abstract
Purpose: A prior Radiation Therapy Oncology Group (RTOG) clinical trial in anaplastic oligodendroglioma suggested a progression-free survival benefit for procarbazine, lomustine, and vincristine (PCV) chemotherapy in addition to radiation therapy (RT), as have smaller trials in low-grade glioma (LGG).
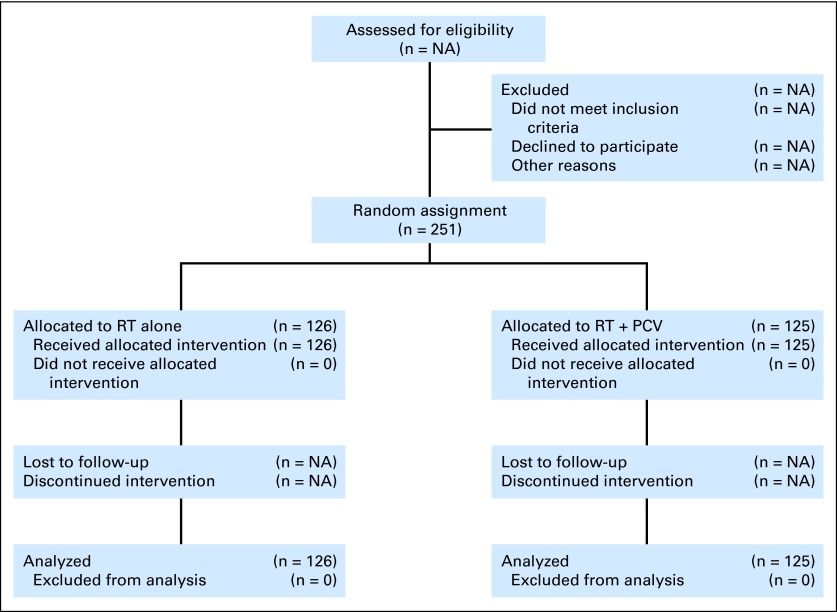
Patients and methods: Eligibility criteria included supratentorial WHO grade 2 LGG, age 18 to 39 years with subtotal resection/biopsy, or age ≥ 40 years with any extent resection. Patients were randomly assigned to RT alone or RT followed by six cycles of PCV. Survival was compared by using the modified Wilcoxon and log-rank tests.
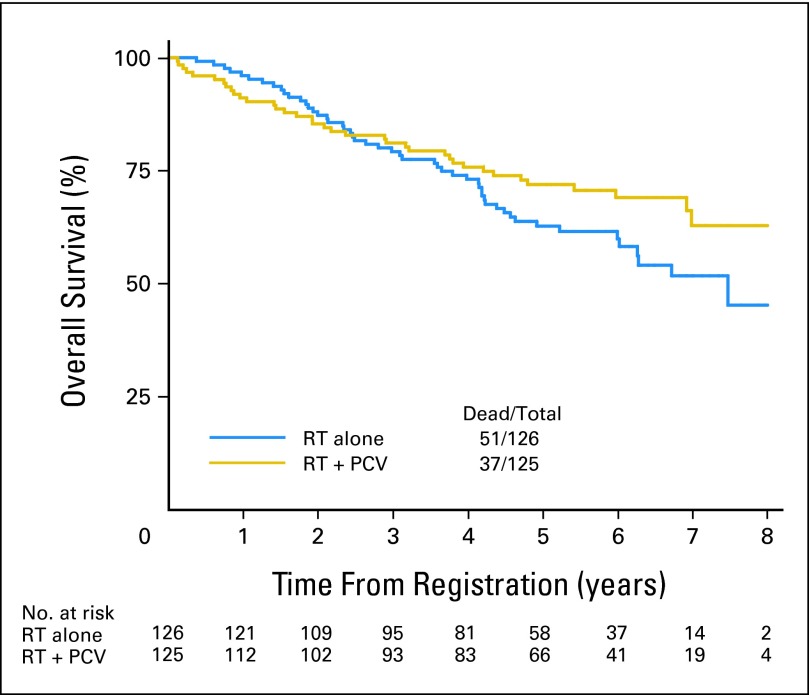
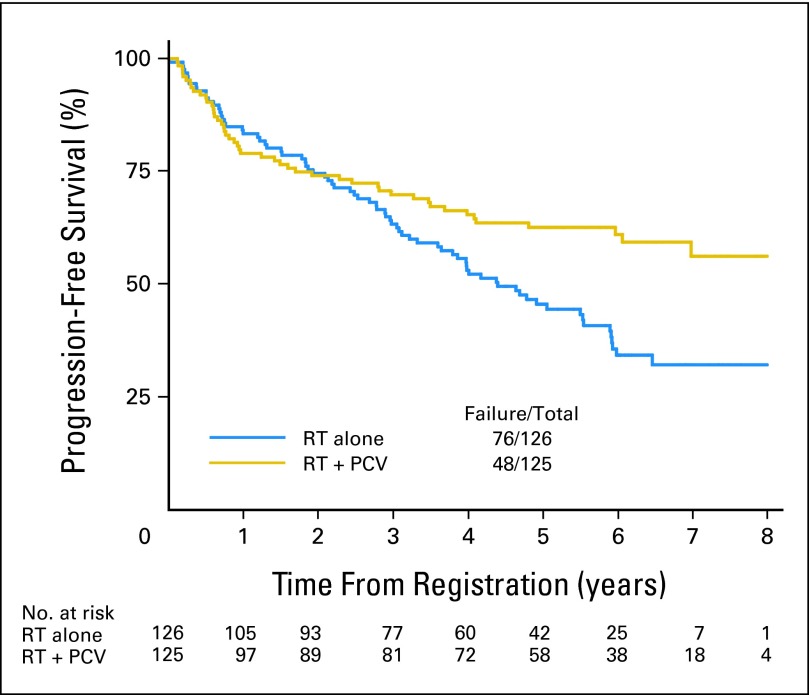
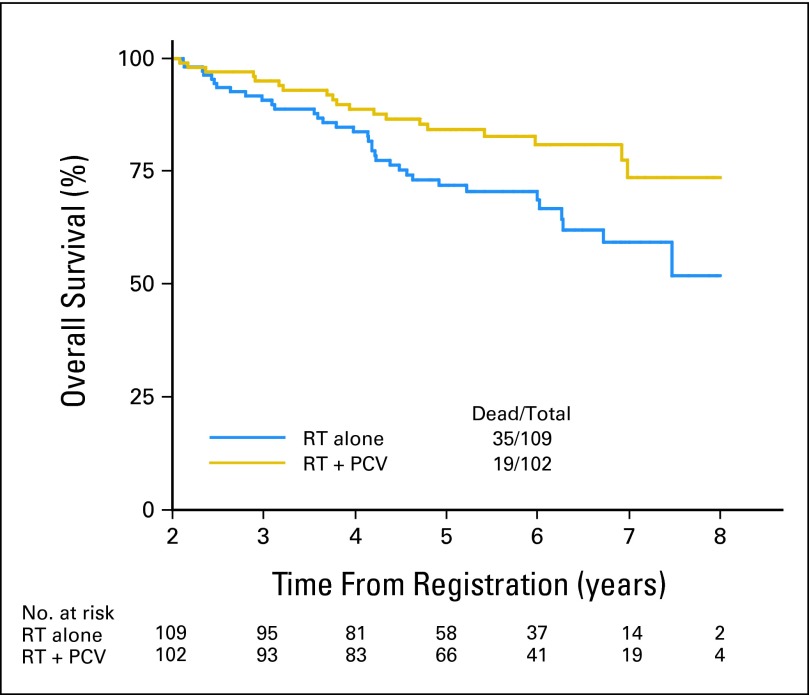
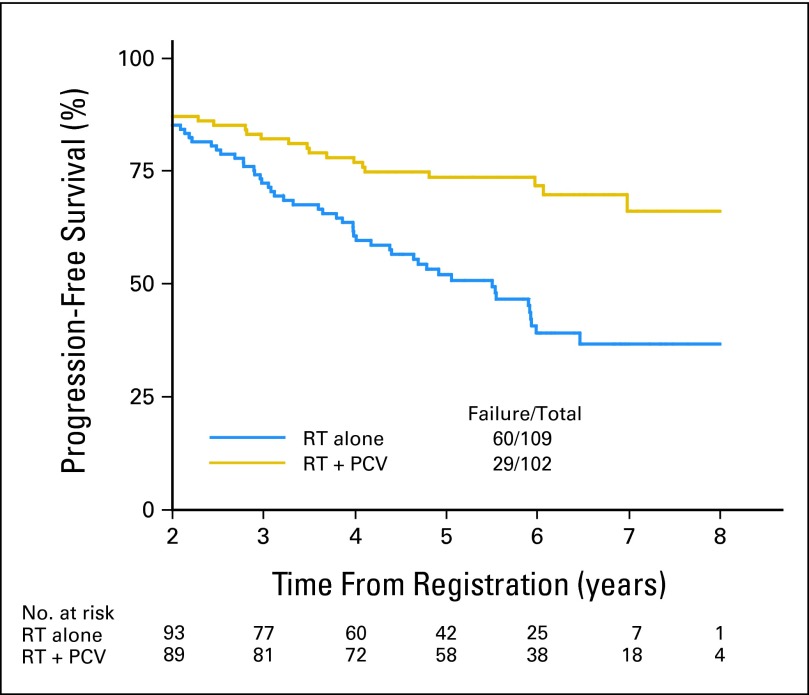
Results: In all, 251 patients were accrued from 1998 to 2002. Median overall survival (OS) time and 5-year OS rates for RT versus RT + PCV were 7.5 years versus not reached and 63% versus 72%, respectively (hazard ratio [HR]; 0.72; 95% CI, 0.47 to 1.10; P = .33; log-rank P = .13). Median progression-free survival (PFS) time and 5-year PFS rates for RT versus RT + PCV were 4.4 years versus not reached and 46% versus 63%, respectively (HR, 0.6; 95% CI, 0.41 to 0.86; P = .06; log-rank P = .005). OS and PFS were similar for all patients between years 0 and 2. After 2 years, OS and PFS curves separated significantly, favoring RT + PCV. For 2-year survivors (n = 211), the probability of OS for an additional 5 years was 74% with RT + PCV versus 59% with RT alone (HR, 0.52; 95% CI, 0.30 to 0.90; log-rank P = .02).
Conclusion: PFS but not OS was improved for adult patients with LGG receiving RT + PCV versus RT alone. On post hoc analysis, for 2-year survivors, the addition of PCV to RT conferred a survival advantage, suggesting a delayed benefit for chemotherapy.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
RTOG 9802: good wines need aging.J Clin Oncol. 2013 Feb 10;31(5):653-4. doi: 10.1200/JCO.2012.46.6896. Epub 2013 Jan 7. J Clin Oncol. 2013. PMID: 23295798 No abstract available.
-
Does RTOG 9802 change practice with respect to newly diagnosed low-grade glioma?J Clin Oncol. 2013 Feb 10;31(5):652-3. doi: 10.1200/JCO.2012.46.7969. Epub 2013 Jan 7. J Clin Oncol. 2013. PMID: 23295807 No abstract available.
-
[Conventionally fractioned postoperative radiotherapy up to 50.4 Gy for progressive low-grade gliomas in adults still standard treatment].Strahlenther Onkol. 2013 Apr;189(4):340-1. doi: 10.1007/s00066-012-0293-y. Strahlenther Onkol. 2013. PMID: 23404142 German. No abstract available.
-
A Randomized Clinical Trial of Radiation With or Without Chemotherapy for Low-grade Gliomas.Neurosurgery. 2016 Oct;79(4):N17-8. doi: 10.1227/01.neu.0000499709.51090.ea. Neurosurgery. 2016. PMID: 27635971 No abstract available.
References
-
- Kleihues P, Burger PC, Scheithauer BW. Histological Typing of Tumours of the Central Nervous System. ed 2. Berlin, Germany: Springer; 1993.
-
- Hinsdale, IL: CBRTUS; 2006. Central Brain Tumor Registry of the United States (CBTRUS): Statistical Report: Primary Brain Tumors in the United States, 1998-2002. http://www.cbtrus.org/reports/2005-2006/2006report.pdf.
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–130. - PubMed
-
- Brown PD, Shaw EG. Low-grade gliomas. In: Gunderson LL, Tepper JE, editors. Clinical Radiation Oncology. ed 2. Philadelphia, PA: Churchill-Livingstone; 2006. pp. 493–514.
-
- van den Bent MJ, Afra D, de Witte O, et al. Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: The EORTC 22845 randomised trial. Lancet. 2005;366:985–990. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
