

Deterioration of neurobehavioral performance in resident physicians during repeated exposure to extended duration work shifts
- PMID: 22851809
- PMCID: PMC3397817
- DOI: 10.5665/sleep.2004
Deterioration of neurobehavioral performance in resident physicians during repeated exposure to extended duration work shifts
Abstract
Study objectives: Although acute sleep loss during 24- to 30-h extended duration work shifts (EDWS) has been shown to impair the performance of resident physicians, little is known about the effects of cumulative sleep deficiency on performance during residency training. Chronic sleep restriction induces a gradual degradation of neurobehavioral performance and exacerbates the effects of acute sleep loss in the laboratory, yet the extent to which this occurs under real-world conditions is unknown. In this study, the authors quantify the time course of neurobehavioral deterioration due to repeated exposure to EDWS during a 3-week residency rotation.
Design: A prospective, repeated-measures, within-subject design.
Setting: Medical and cardiac intensive care units, Brigham and Women's Hospital, Boston, MA.
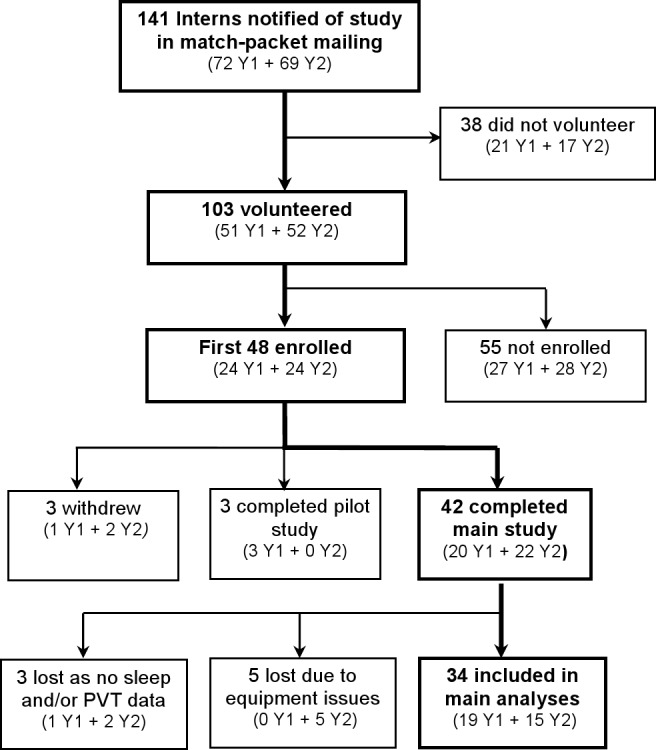
Participants: Thirty-four postgraduate year one resident physicians (23 males; age 28.0 ± 1.83 (standard deviation) years)
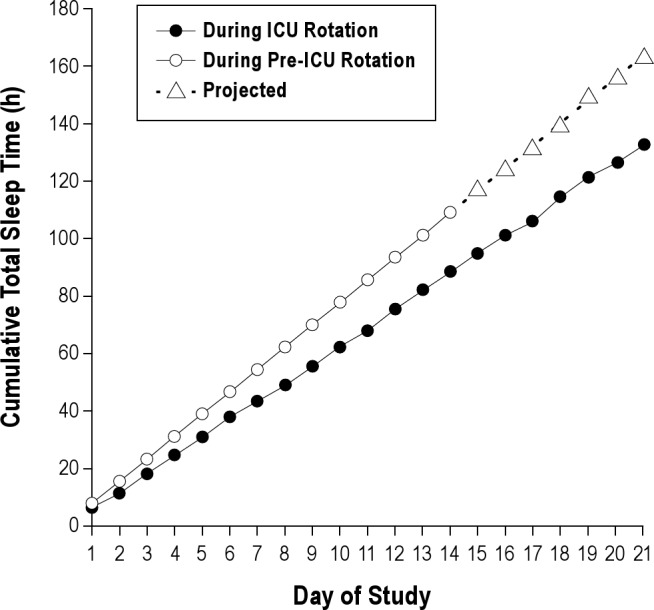
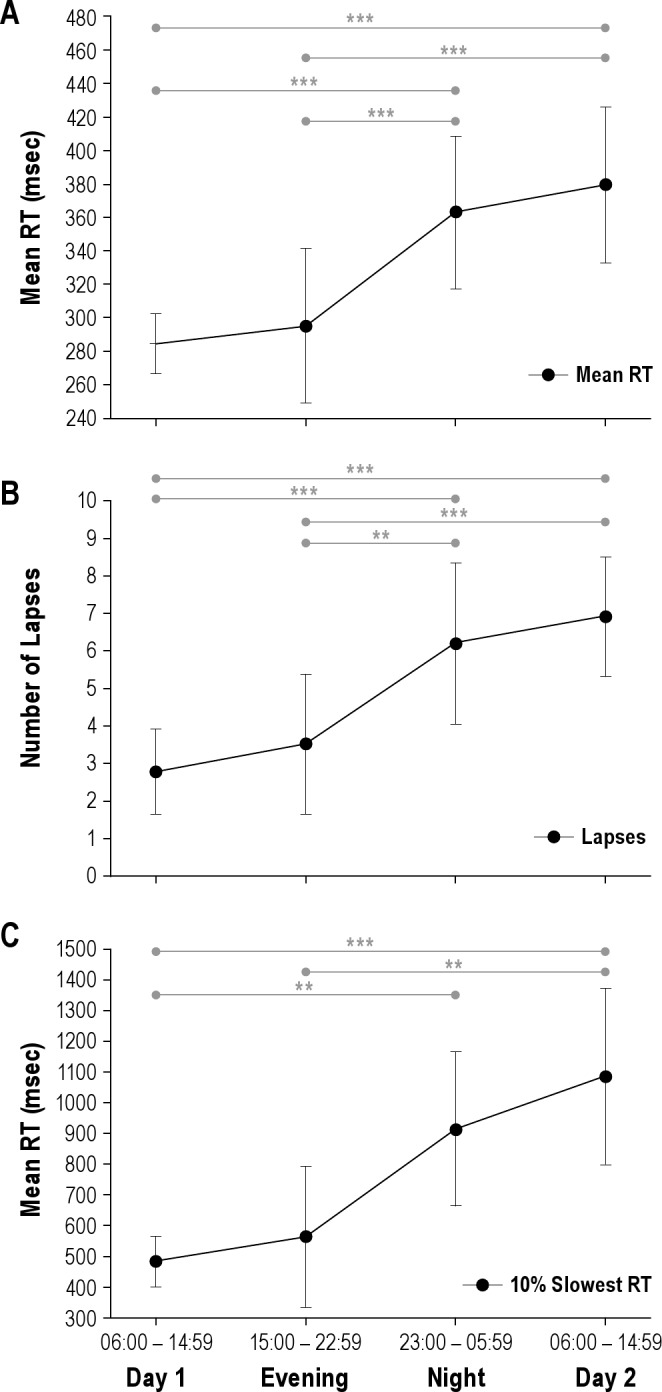
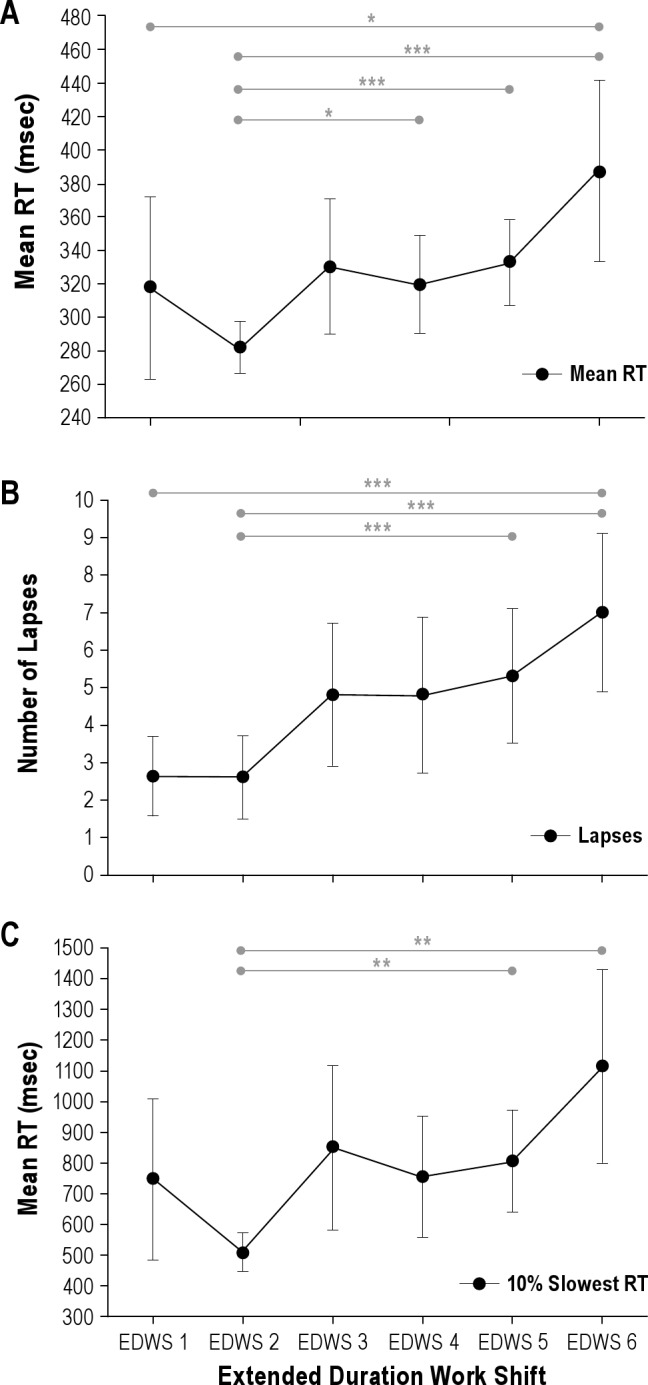
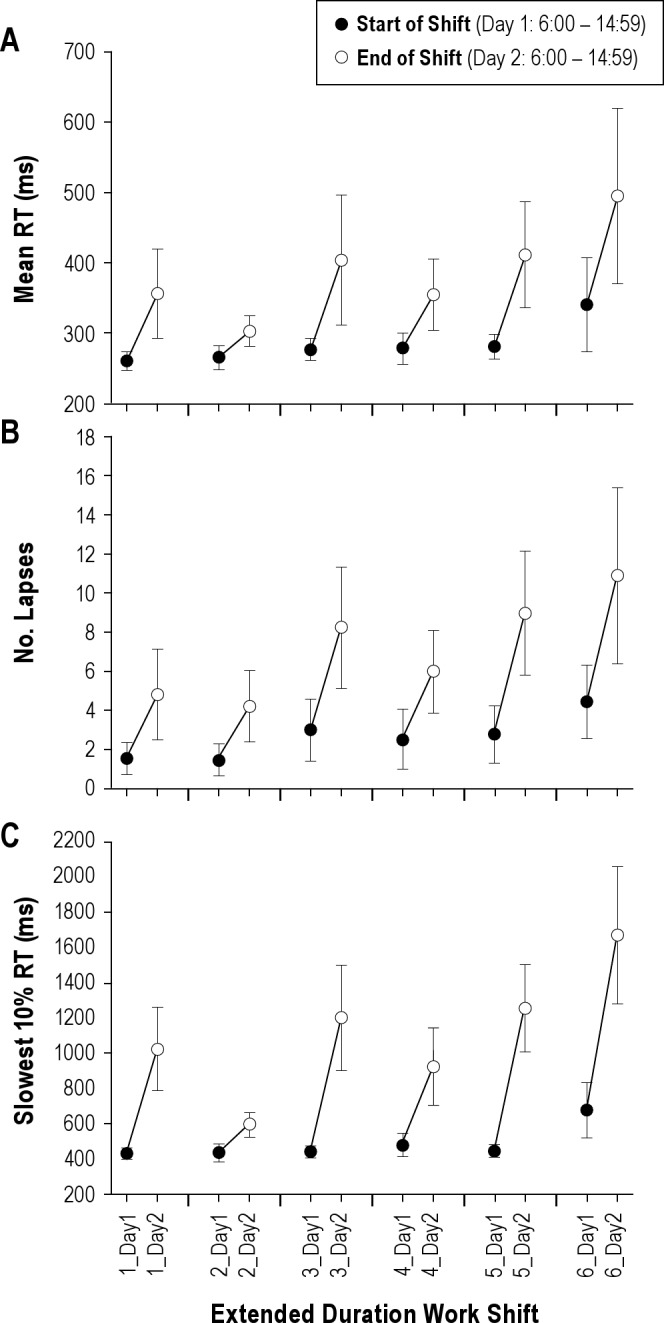
Measurements and results: Residents working a 3-week Q3 schedule (24- to 30-h work shift starts every 3(rd) day), consisting of alternating 24- to 30-h (EDWS) and approximately 8-h shifts, underwent psychomotor vigilance testing before, during, and after each work shift. Mean response time, number of lapses, and slowest 10% of responses were calculated for each test. Residents also maintained daily sleep/wake/work logs. EDWS resulted in cumulative sleep deficiency over the 21-day rotation (6.3 h sleep obtained per day; average 2.3 h sleep obtained per extended shift). Response times deteriorated over a single 24- to 30-h shift (P < 0.0005), and also cumulatively with each successive EDWS: Performance on the fifth and sixth shift was significantly worse than on the first shift (P < 0.01). Controlling for time of day, there was a significant acute (time on shift) and chronic (successive EDWS) interaction on psychomotor vigilance testing response times (P < 0.05).
Conclusions: Chronic sleep deficiency caused progressive degradation in residents' neurobehavioral performance and exacerbated the effects of acute sleep loss inherent in the 24- to 30-h EDWS that are commonly used in resident schedules.
Keywords: Extended duration work shift; acute; chronic; graduate medical education; psychomotor vigilance test; resident; sleep deficiency.
Figures
References
-
- Ulmer C, Wolman D, Johns M Committee on Optimizing Graduate Medical Trainee (Resident) Hours and Work Schedules to Improve Patient Safety for the Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Washington, D.C: The National Academies Press; 2008. - PubMed
-
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Engl J Med. 2004;351:1838–48. - PubMed
-
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294:1025–33. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
