

Phalloplasty in complete aphallia and ambiguous genitalia
- PMID: 22851911
- PMCID: PMC3312182
- DOI: 10.1055/s-0031-1281489
Phalloplasty in complete aphallia and ambiguous genitalia
Abstract
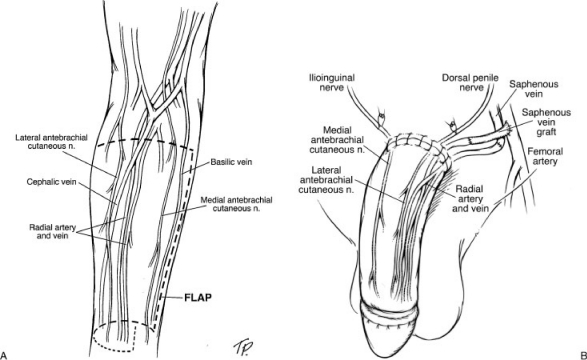
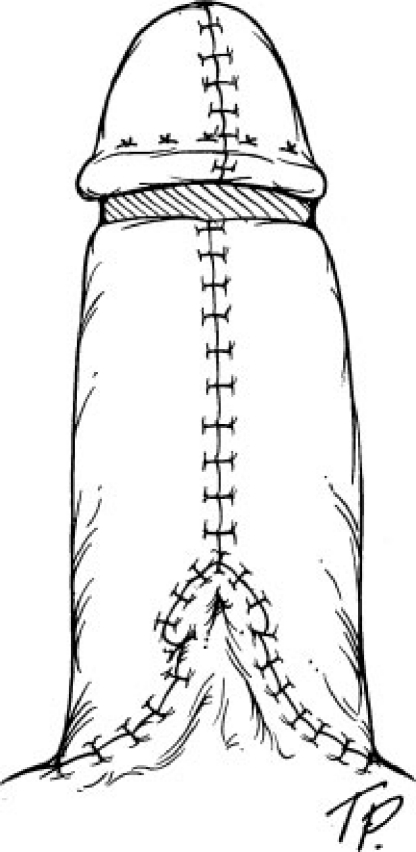
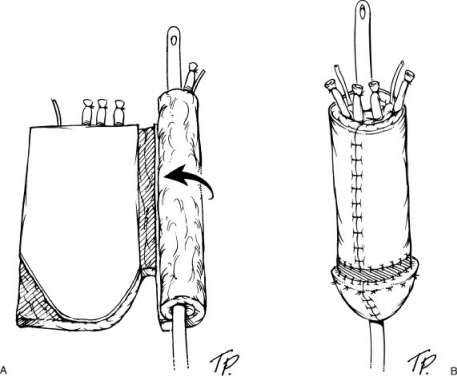
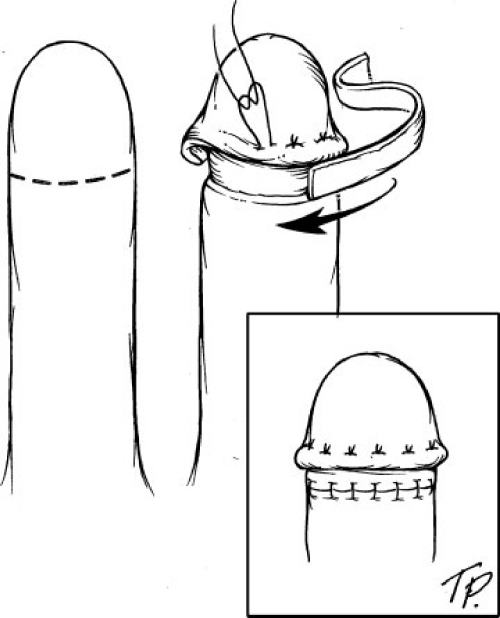
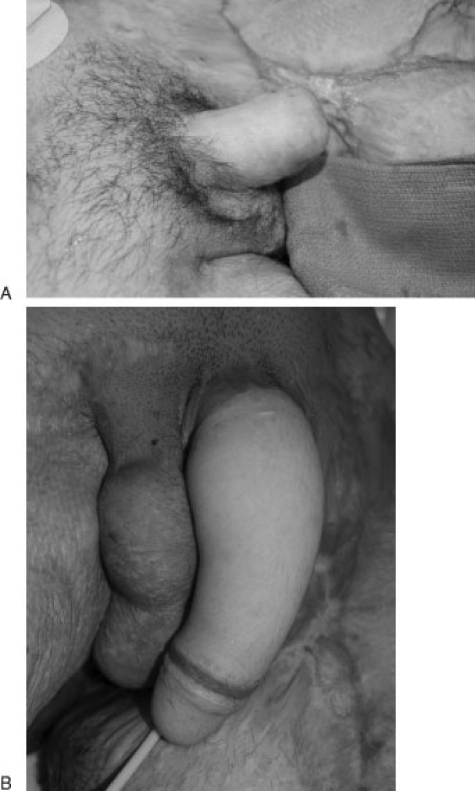
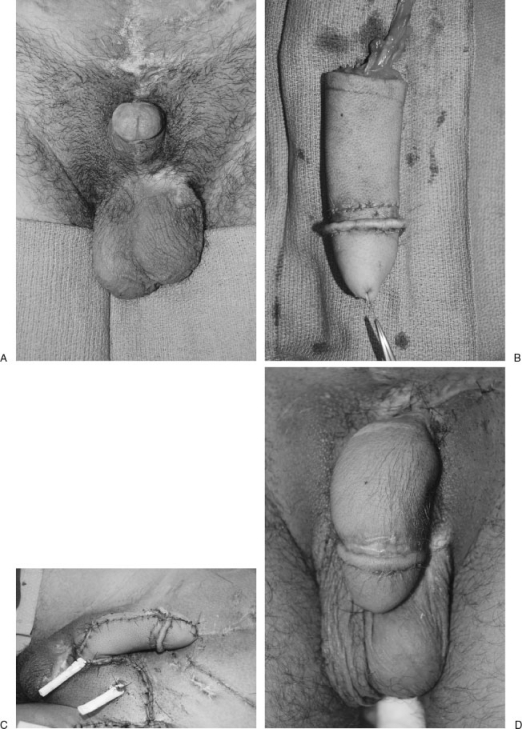
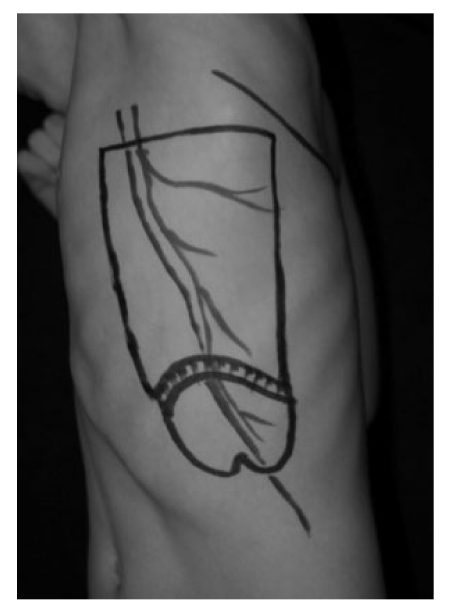
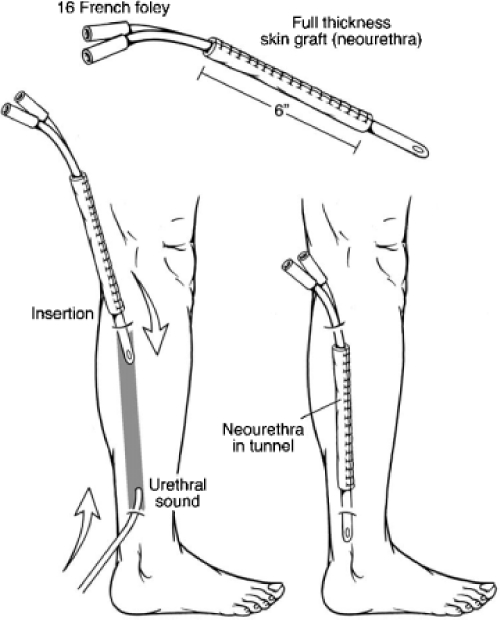
The most common indications for phalloplasty in children include aphallia, micropenis/severe penile inadequacy, ambiguous genitalia, phallic inadequacy associated with epispadias/bladder exstrophy and female to male gender reassignment in adolescents. There are many surgical options for phalloplasty; both local pedicled tissue as well as free tissue transfer. The advantages of local tissue include a more concealed donor site, less complex operation and potentially faster recovery. However, pedicled options are generally less sensate, making placement of a penile prosthesis more risky and many children with bladder exstrophy have been previously operated upon making the blood supply for local pedicled flaps less reliable. This Here the authors discuss free tissue transfer, including the radial forearm, the anterolateral thigh, the scapula and latissimus, and the fibula free flaps, as well as local rotational flaps from the abdomen, groin, and thigh. The goal of reconstruction should be an aesthetic and functional (ability to penetrate) phallus, which provides tactile and erogenous sensation, and the ability to urinate standing. Ideally, the operation should be completed in one to two operations with minimal donor site morbidity. There are advantages and disadvantages of each of flap and thus the choice of donor site should be a combination of the patient's preference and surgeon's ability to produce a consistent result.
Keywords: Phalloplasty; aphallia; children bladder exstrophy.
Figures



Similar articles
-
Pedicled Anterolateral Thigh and Radial Forearm Free Flap Phalloplasty for Penile Reconstruction in Patients With Bladder Exstrophy.J Urol. 2021 Mar;205(3):880-887. doi: 10.1097/JU.0000000000001404. Epub 2020 Oct 7. J Urol. 2021. PMID: 33026935
-
Radial forearm free flap phalloplasty for penile inadequacy in patients with exstrophy.J Urol. 2013 Oct;190(4 Suppl):1577-82. doi: 10.1016/j.juro.2012.12.050. Epub 2012 Dec 25. J Urol. 2013. PMID: 23270911
-
Microsurgical Gender Affirmation Surgery.Semin Plast Surg. 2022 Nov 11;36(4):274-284. doi: 10.1055/s-0042-1758226. eCollection 2022 Nov. Semin Plast Surg. 2022. PMID: 36561429 Free PMC article. Review.
-
Substitution Phalloplasty in Patients With Bladder Exstrophy-Epispadias Complex: A Systematic Review of Techniques, Complications and Outcomes.J Sex Med. 2021 Feb;18(2):400-409. doi: 10.1016/j.jsxm.2020.10.007. Epub 2020 Nov 20. J Sex Med. 2021. PMID: 33223423
-
Reconstructive surgery for severe penile inadequacy: phalloplasty with a free radial forearm flap or a pedicled anterolateral thigh flap.Adv Urol. 2008;2008:704343. doi: 10.1155/2008/704343. Epub 2008 Nov 4. Adv Urol. 2008. PMID: 19009034 Free PMC article.
Cited by
-
Mystery and realities of phalloplasty: a systematic review.Turk J Urol. 2017 Sep;43(3):229-236. doi: 10.5152/tud.2017.14554. Epub 2017 Aug 3. Turk J Urol. 2017. PMID: 28861290 Free PMC article. Review.
-
Minimising the donor area morbidity of radial forearm phalloplasty using prefabricated thigh flap: A new technique.Indian J Plast Surg. 2017 Jan-Apr;50(1):91-95. doi: 10.4103/ijps.IJPS_158_16. Indian J Plast Surg. 2017. PMID: 28615818 Free PMC article.
-
Latissimus dorsi free flap phalloplasty: a systematic review.Int J Impot Res. 2020 Nov;33(7):746-753. doi: 10.1038/s41443-020-00371-x. Epub 2020 Nov 12. Int J Impot Res. 2020. PMID: 33184508
-
"Bird-Wing" abdominal phalloplasty: A novel surgical technique for penile reconstruction.J Indian Assoc Pediatr Surg. 2013 Apr;18(2):49-52. doi: 10.4103/0971-9261.109351. J Indian Assoc Pediatr Surg. 2013. PMID: 23798805 Free PMC article.
-
Inflatable penile prosthesis technique and outcomes after radial forearm free flap neophalloplasty.Int J Impot Res. 2015 Mar-Apr;27(2):49-53. doi: 10.1038/ijir.2014.30. Epub 2014 Aug 7. Int J Impot Res. 2015. PMID: 25099636
References
-
- Gearhart J, Mathews R. Wein A J, Kavoussi L R, Novick A C, Partin A W. Campbell-Walsh Urology. 9th ed. Philadelphia: Saunders; 2007. Exstrophy/epispadias; pp. 3497–3555.
-
- Salgado C J, Monstrey S, Hoebeke P, Lumen N, Dwyer M, Mardini S. Reconstruction of the penis after surgery. Urol Clin North Am. 2010;37(3):379–401. - PubMed
-
- Monstrey S, Hoebeke P, Selvaggi G, et al. Penile reconstruction: is the radial forearm flap really the standard technique? Plast Reconstr Surg. 2009;124(2):510–518. - PubMed
-
- Bogoras N. Plastic construction penis capable of accomplishing coitus. Zentralbl Chir. 1936;63:1271–1276.
-
- Song R, Gao Y, Song Y, Yu Y, Song Y. The forearm flap. Clin Plast Surg. 1982;9(1):21–26. - PubMed
LinkOut - more resources
Full Text Sources
Medical
