

Scrotal and perineal reconstruction
- PMID: 22851913
- PMCID: PMC3312186
- DOI: 10.1055/s-0031-1281491
Scrotal and perineal reconstruction
Abstract
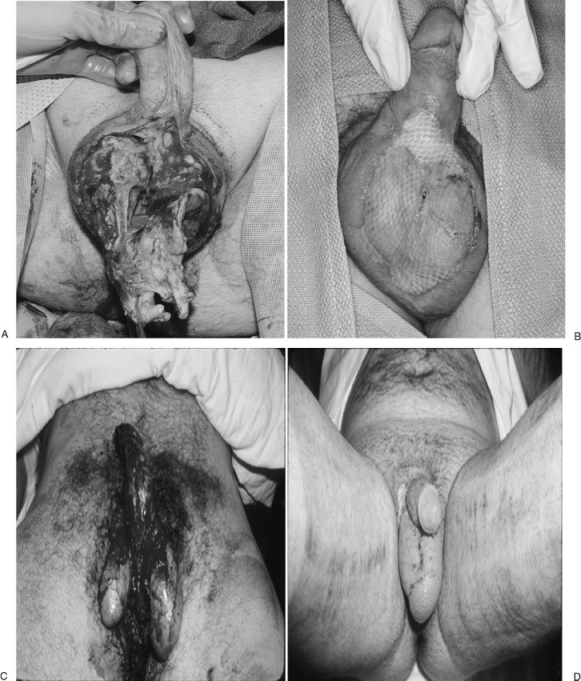
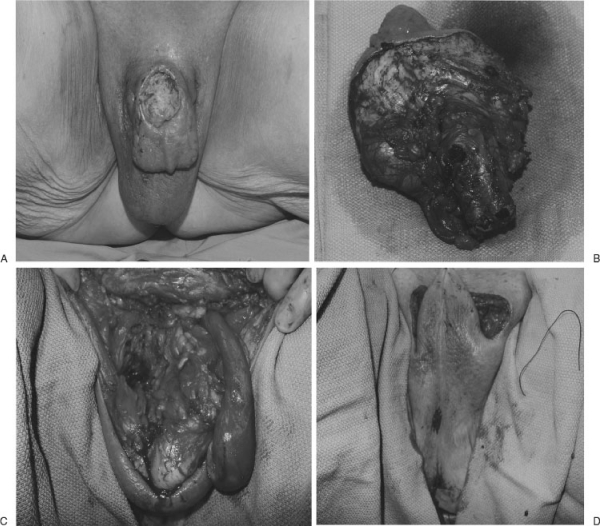
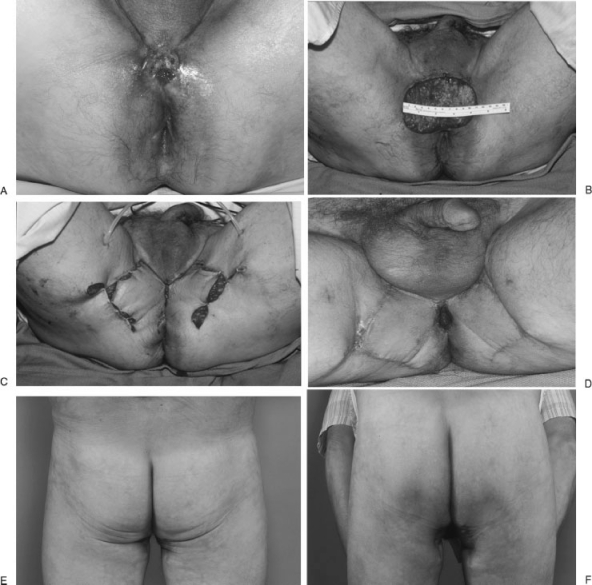
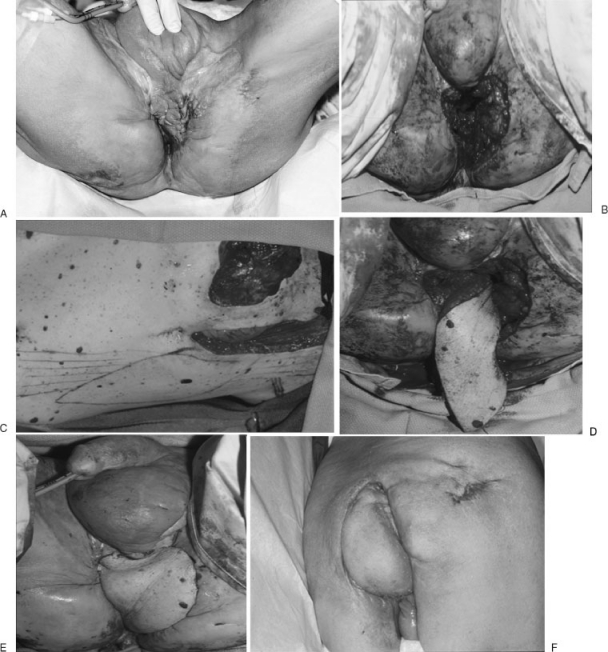
The scrotal and perineal area serves a special function. It is the pelvic outlet for the gastrointestinal tract, urinary system, and sexual function. In the male, the scrotum allows testicular mobility to reduce trauma and allow optimal thermal regulation for spermatogenesis. Trauma, infection, and cancer resection create defects that require reconstruction. The reconstructive goal here is to obtain durable coverage, function, and lastly aesthetic outcome. Pedicled local and regional flaps are the mainstay for this area. Due to the special function and appearance of the scrotum, reconstructive options for total scrotal defect always fall far short of the native scrotum. On the other hand, perineal reconstruction is overall satisfactory.
Keywords: Scrotal wound; flap coverage; perineal wound.
Figures

Similar articles
-
Scrotal flap for closure of perineal skin defects in dogs.Vet Surg. 2013 Feb;42(2):186-91. doi: 10.1111/j.1532-950X.2012.00998.x. Epub 2012 Jul 23. Vet Surg. 2013. PMID: 22823187
-
Crafting Contours: A Comprehensive Guide to Scrotal Reconstruction.Life (Basel). 2024 Feb 4;14(2):223. doi: 10.3390/life14020223. Life (Basel). 2024. PMID: 38398732 Free PMC article. Review.
-
Reconstruction of scrotal and perineal defects in Fournier's gangrene.J Plast Reconstr Aesthet Surg. 2011 Apr;64(4):528-34. doi: 10.1016/j.bjps.2010.07.018. Epub 2010 Aug 24. J Plast Reconstr Aesthet Surg. 2011. PMID: 20797927
-
Reconstruction of Defects After Fournier Gangrene: A Systematic Review.Eplasty. 2015 May 26;15:e18. eCollection 2015. Eplasty. 2015. PMID: 26171090 Free PMC article. Review.
-
SCROTAL RECONSTRUCTION WITH A PEDICLED GRACILIS MUSCLE FLAP AFTER DEBRIDEMENT OF FOURNIER'S GANGRENE: A CASE REPORT.East Afr Med J. 2013 Nov;90(11):375-8. East Afr Med J. 2013. PMID: 26862639
Cited by
-
The versatility of the medial thigh lift for defect coverage in the genito-perineal region.Int Wound J. 2017 Jun;14(3):496-500. doi: 10.1111/iwj.12634. Epub 2016 Aug 1. Int Wound J. 2017. PMID: 27476473 Free PMC article.
-
[Reconstructive methods after Fournier gangrene].Urologe A. 2016 Apr;55(4):484-8. doi: 10.1007/s00120-015-4001-2. Urologe A. 2016. PMID: 26649739 Review. German.
-
Multivariate analysis of early surgical management factors affecting posttraumatic penoscrotal avulsion injury: a level I trauma center study.BMC Urol. 2021 Jan 7;21(1):7. doi: 10.1186/s12894-020-00763-7. BMC Urol. 2021. PMID: 33413250 Free PMC article.
-
Rectal cancer and Fournier's gangrene - current knowledge and therapeutic options.World J Gastroenterol. 2015 Aug 14;21(30):9002-20. doi: 10.3748/wjg.v21.i30.9002. World J Gastroenterol. 2015. PMID: 26290629 Free PMC article. Review.
-
The superomedial thigh flap in scrotal reconstruction: Technical steps to improve cosmetic results.Indian J Urol. 2013 Oct;29(4):360-2. doi: 10.4103/0970-1591.120132. Indian J Urol. 2013. PMID: 24235804 Free PMC article.
References
-
- Jung A, Schuppe H C. Influence of genital heat stress on semen quality in humans. Andrologia. 2007;39(6):203–215. - PubMed
-
- Werdelin L, Nilsonne Å. The evolution of the scrotum and testicular descent in mammals: a phylogenetic view. J Theor Biol. 1999;196(1):61–72. - PubMed
-
- Grayson D E, Abbott R M, Levy A D, Sherman P M. Emphysematous infections of the abdomen and pelvis: a pictorial review. Radiographics. 2002;22(3):543–561. - PubMed
-
- Levenson R B, Singh A K, Novelline R A. Fournier gangrene: role of imaging. Radiographics. 2008;28(2):519–528. - PubMed
-
- Yaghan R J, Al-Jaberi T M, Bani-Hani I. Fournier's gangrene: changing face of the disease. Dis Colon Rectum. 2000;43(9):1300–1308. - PubMed
