

Temporal lobe abscess in a patient with isolated sphenoiditis
- PMID: 22852114
- PMCID: PMC3390129
- DOI: 10.2500/ar.2011.2.0001
Temporal lobe abscess in a patient with isolated sphenoiditis
Abstract
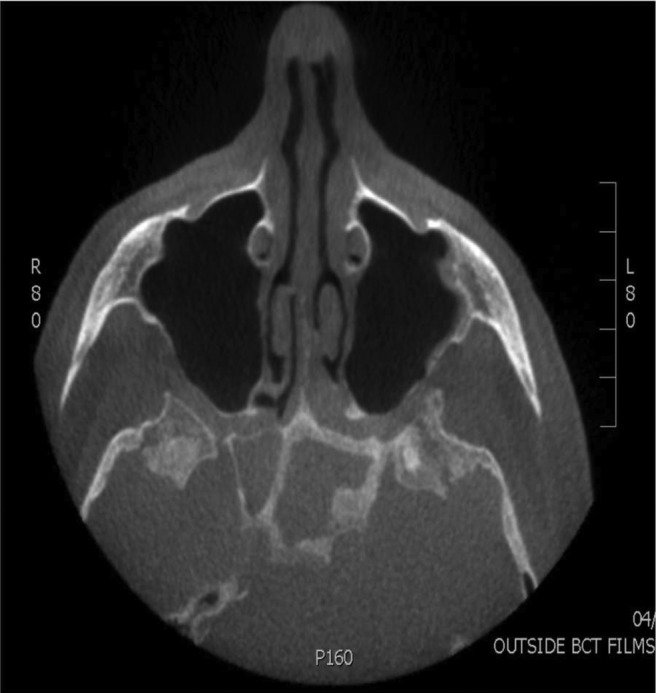
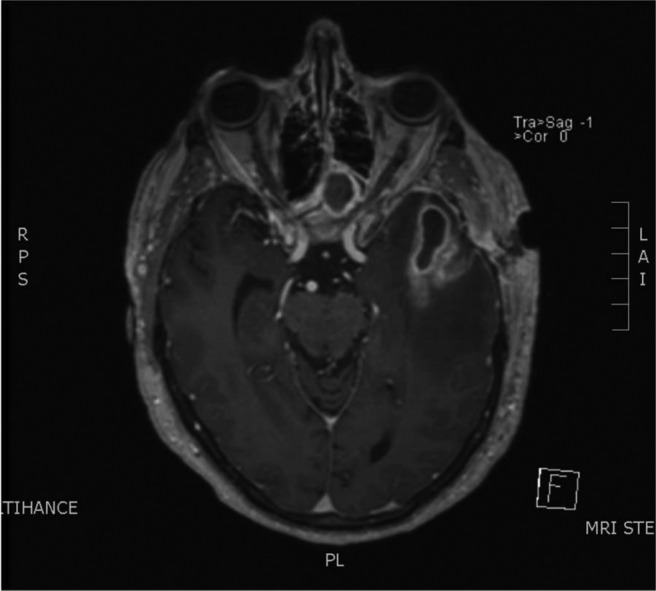
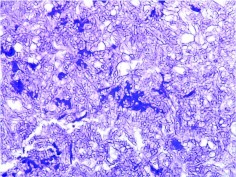
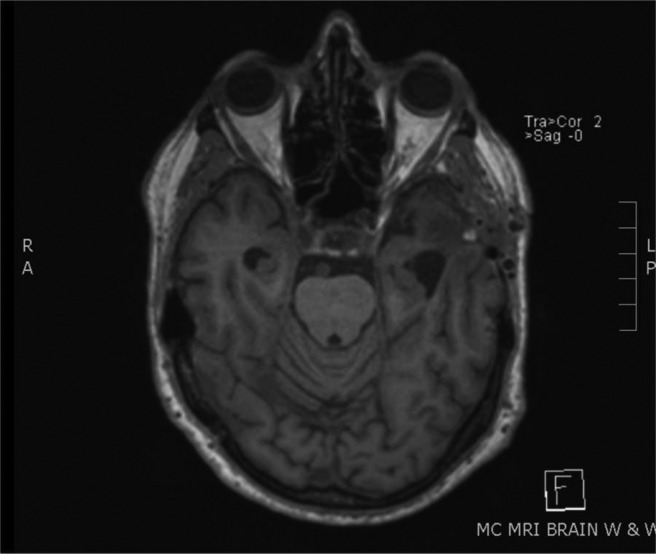
A 74-year-old immunocompetent man admitted for severe retro-orbital headache was diagnosed with isolated sphenoiditis. At the time of scheduled surgery, the patient was mildly obtunded, and a head CT revealed a temporal lobe abscess. The patient underwent a left temporal craniectomy and a bilateral endoscopic sphenoid sinusotomy, which revealed gross fungal debris. The patient made a full recovery with resolution of abscess and sinus findings. Suspicion for intracranial infection should be raised in any sinus patient with neurological changes. Early diagnosis with imaging studies is extremely important for surgical drainage before permanent neurological sequelae.
Keywords: Abcess; allergic sinusitis; fungal infection; headache; sinonasal; sphenoiditis; temporal lobe.
Conflict of interest statement
The authors have no conflicts to declare pertaining to this article
Figures


Similar articles
-
Chronic Sphenoiditis With Deep Neck Space Extension: Case Report With Review of the Literature and Postulated Mechanisms for Extracranial Extension.Ear Nose Throat J. 2024 Mar;103(3):151-155. doi: 10.1177/0145561321989453. Epub 2021 Jan 20. Ear Nose Throat J. 2024. PMID: 33470832 Review.
-
[Neurological manifestations of isolated sphenoiditis].Zhonghua Yi Xue Za Zhi. 2001 Aug 25;81(16):988-90. Zhonghua Yi Xue Za Zhi. 2001. PMID: 11718083 Chinese.
-
Twelve-year-old girl with intracranial epidural abscess and sphenoiditis.Brain Dev. 2014 Apr;36(4):359-61. doi: 10.1016/j.braindev.2013.06.001. Epub 2013 Jun 29. Brain Dev. 2014. PMID: 23815969
-
Invasive fungal sinusitis of the sphenoid sinus.Clin Exp Otorhinolaryngol. 2014 Sep;7(3):181-7. doi: 10.3342/ceo.2014.7.3.181. Epub 2014 Aug 1. Clin Exp Otorhinolaryngol. 2014. PMID: 25177433 Free PMC article.
-
Nasal septal abscess complicating isolated acute sphenoiditis: case report and literature review.B-ENT. 2010;6(4):303-5. B-ENT. 2010. PMID: 21302696 Review.
Cited by
-
Isolated Sphenoid Sinus Lesions: Experience with a Few Rare Pathologies.J Neurosci Rural Pract. 2017 Jan-Mar;8(1):107-113. doi: 10.4103/0976-3147.193540. J Neurosci Rural Pract. 2017. PMID: 28149092 Free PMC article.
-
Isolated Acute Sphenoid Fungal Sinusitis with Cavernous Sinus Thrombosis: Our Experience.Indian J Otolaryngol Head Neck Surg. 2022 Oct;74(Suppl 2):987-993. doi: 10.1007/s12070-020-02059-6. Epub 2020 Aug 19. Indian J Otolaryngol Head Neck Surg. 2022. PMID: 36452689 Free PMC article.
-
Expressive aphasia caused by Streptococcus intermedius brain abscess in an immunocompetent patient.Int Med Case Rep J. 2017 Jan 23;10:25-30. doi: 10.2147/IMCRJ.S125684. eCollection 2017. Int Med Case Rep J. 2017. PMID: 28176963 Free PMC article.
References
-
- Epstein VA, Kern RC. Invasive fungal sinusitis and complications of rhinosinusitis. Otolaryngol Clin North Am 41:497–524, viii, 2008 - PubMed
-
- Lin JJ, Wu CT, Hsia SH, et al. Pneumocephalus: A rare presentation of Candida sphenoid sinusitis. Pediatr Neurol 40:398–400, 2009 - PubMed
-
- Chopra H, Dua K, Malhotra V, et al. Invasive fungal sinusitis of isolated sphenoid sinus in immunocompetent subjects. Mycoses 49:30–36, 2006 - PubMed
-
- Sridhara SR, Paragache G, Panda NK, Chakrabarti A. Mucormycosis in immunocompetent individuals: An increasing trend. J Otolaryngol 34:402–406, 2005 - PubMed
-
- Anselmo-Lima WT, Lopes RP, Valera FC, Demarco RC. Invasive fungal rhinosinusitis in immunocompromised patients. Rhinology 42:141–144, 2004 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
