

Therapeutic concentrations of antibiotics inhibit Shiga toxin release from enterohemorrhagic E. coli O104:H4 from the 2011 German outbreak
- PMID: 22853739
- PMCID: PMC3438081
- DOI: 10.1186/1471-2180-12-160
Therapeutic concentrations of antibiotics inhibit Shiga toxin release from enterohemorrhagic E. coli O104:H4 from the 2011 German outbreak
Abstract
Background: The shiga toxin-producing E. coli (STEC) O104:H4 caused a major outbreak in Germany in spring 2011. STEC are usually susceptible to common antibiotics. However, antibiotic treatment of STEC-infected patients is not recommended because STEC may enhance production and release of shiga toxins (STX) in response to antibiotics, which eventually enhances the frequency and severity of clinical symptoms, including haemolytic uraemic syndrome (HUS) and fatalities.
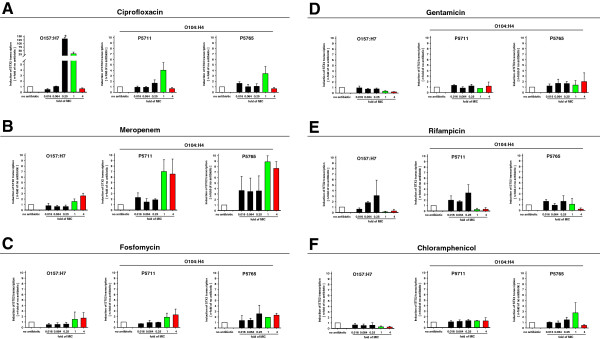
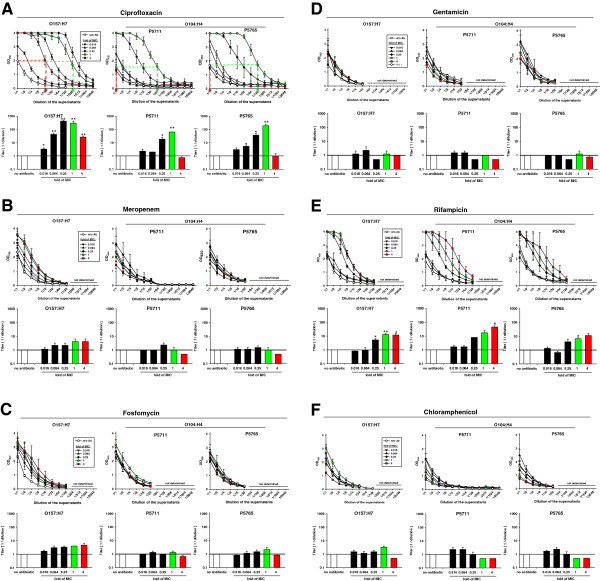
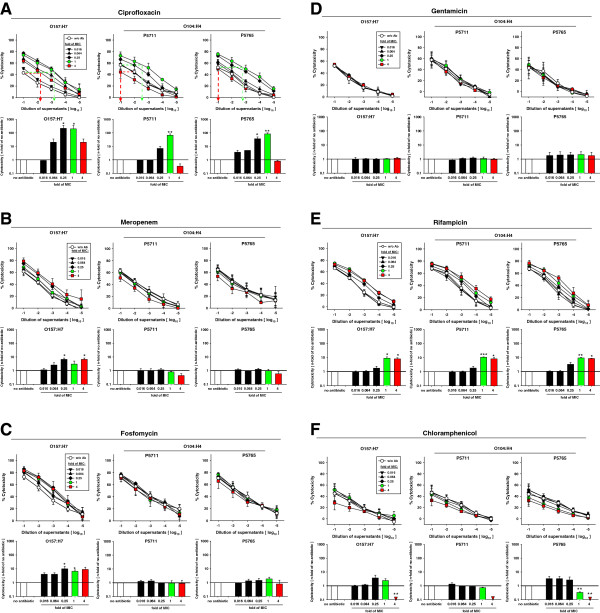
Results: We characterized the response to antibiotics of STEC O104:H4 isolates from two HUS patients during the German STEC outbreak in spring 2011 in comparison to the common STEC O157:H7. Liquid cultures of STEC O157:H7 and O104:H4 were incubated with graded dilutions of the antibiotics ciprofloxacin, meropenem, fosfomycin, gentamicin, rifampicin, and chloramphenicol. At defined times of antibiotic treatment, transcriptional activation of the STX2 gene, contents of STX and STX-activity in the culture supernatants were quantified. Unlike the common serotype O157:H7, STEC O104:H4 does not release STX in response to therapeutic concentrations of ciprofloxacin, meropenem, fosfomycin, and chloramphenicol.
Conclusions: In future outbreaks, the response of the respective epidemiologic STEC strain to antibiotics should be rapidly characterized in order to identify antibiotics that do not enhance the release of STX. This will eventually allow clinical studies tackling the question whether antibiotic treatment impacts on the eradication of STEC, clinical course of disease, and frequency of carriers.
Figures
References
-
- Robert Koch Institute. Report: Final presentation and evaluation of epidemiological findings in the EHEC O104:H4 outbreak, Germany 2011. , Berlin; 2011. www.rki.de.
-
- Grif K, Dierich MP, Karch H, Allerberger F. Strain-specific differences in the amount of Shiga toxin released from enterohemorrhagic Escherichia coli O157 following exposure to subinhibitory concentrations of antimicrobial agents. Eur J Clin Microbiol Infect Dis. 1998;17(11):761–766. doi: 10.1007/s100960050181. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
