

Early prediction of histopathological response of rectal tumors after one week of preoperative radiochemotherapy using 18 F-FDG PET-CT imaging. A prospective clinical study
- PMID: 22853868
- PMCID: PMC3447722
- DOI: 10.1186/1748-717X-7-124
Early prediction of histopathological response of rectal tumors after one week of preoperative radiochemotherapy using 18 F-FDG PET-CT imaging. A prospective clinical study
Abstract
Background: Preoperative radiochemotherapy (RCT) is standard in locally advanced rectal cancer (LARC). Initial data suggest that the tumor's metabolic response, i.e. reduction of its 18 F-FDG uptake compared with the baseline, observed after two weeks of RCT, may correlate with histopathological response. This prospective study evaluated the ability of a very early metabolic response, seen after only one week of RCT, to predict the histopathological response to treatment.
Methods: Twenty patients with LARC who received standard RCT regimen followed by radical surgery participated in this study. Maximum standardized uptake value (SUV-MAX), measured by PET-CT imaging at baseline and on day 8 of RCT, and the changes in FDG uptake (ΔSUV-MAX), were compared with the histopathological response at surgery. Response was classified by tumor regression grade (TRG) and by achievement of pathological complete response (pCR).
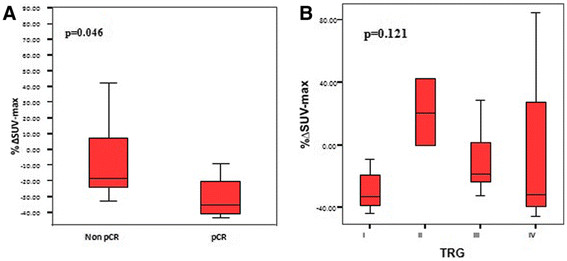
Results: Absolute SUV-MAX values at both time points did not correlate with histopathological response. However, patients with pCR had a larger drop in SUV-MAX after one week of RCT (median: -35.31% vs -18.42%, p = 0.046). In contrast, TRG did not correlate with ΔSUV-MAX. The changes in FGD-uptake predicted accurately the achievement of pCR: only patients with a decrease of more than 32% in SUV-MAX had pCR while none of those whose tumors did not show any decrease in SUV-MAX had pCR.
Conclusions: A decrease in ΔSUV-MAX after only one week of RCT for LARC may be able to predict the achievement of pCR in the post-RCT surgical specimen. Validation in a larger independent cohort is planned.
Figures



References
-
- Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, Rutten HJ, Pahlman L, Glimelius B, van Krieken JH, Leer JW, van de Velde CJ. Dutch Colorectal Cancer Group. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345:638–646. doi: 10.1056/NEJMoa010580. - DOI - PubMed
-
- Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens JH, Liersch T, Schmidberger H, Raab R. German Rectal Cancer Study Group. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–1740. doi: 10.1056/NEJMoa040694. - DOI - PubMed
-
- Valentini V, Coco C, Cellini N, Picciocchi A, Fares MC, Rosetto ME, Mantini G, Morganti AG, Barbaro B, Cogliandolo S, Nuzzo G, Tedesco M, Ambesi-Impiombato F, Cosimelli M, Rotman M. Ten years of preoperative chemoradiation for extraperitoneal T3 rectal cancer: Acute toxicity, tumor response, and sphincter preservation in three consecutive studies. Int J Radiat Oncol Biol Phys. 2001;51:371–383. - PubMed
-
- Capirci C, Rubello D, Chierichetti F, Crepaldi G, Fanti S, Mandoliti G, Salviato S, Boni G, Rampin L, Polico C, Mariani G. Long-term prognostic value of 18 F-FDG PET in patients with locally advanced rectal cancer previously treated with neoadjuvant radiochemotherapy. Am J Roentgenol. 2006;187:W202–W208. doi: 10.2214/AJR.05.0902. - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
