

Locoregional extension patterns of nasopharyngeal carcinoma and suggestions for clinical target volume delineation
- PMID: 22854064
- PMCID: PMC3777458
- DOI: 10.5732/cjc.012.10095
Locoregional extension patterns of nasopharyngeal carcinoma and suggestions for clinical target volume delineation
Abstract
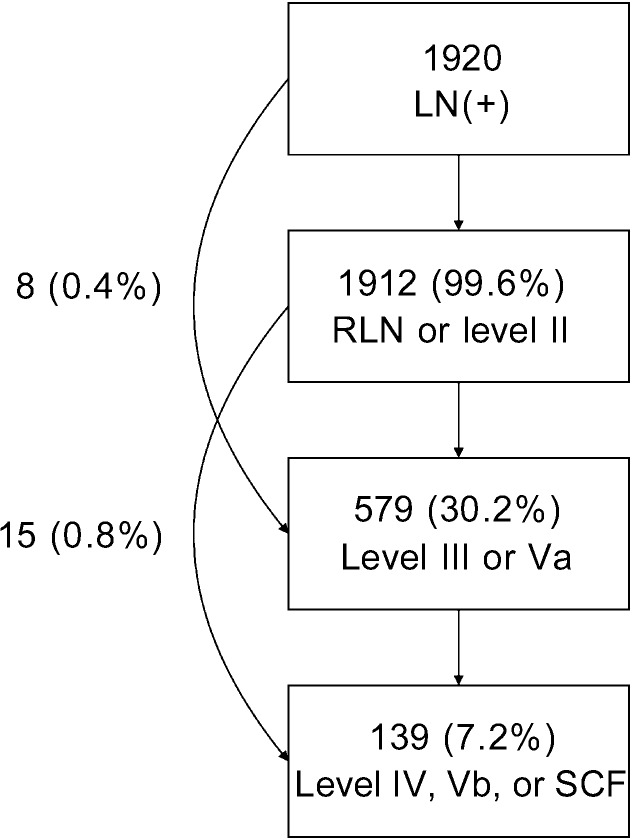
Clinical target volume (CTV) delineation is crucial for tumor control and normal tissue protection. This study aimed to define the locoregional extension patterns of nasopharyngeal carcinoma (NPC) and to improve CTV delineation. Magnetic resonance imaging scans of 2366 newly diagnosed NPC patients were reviewed. According to incidence rates of tumor invasion, the anatomic sites surrounding the nasopharynx were classified into high-risk (>30%), medium-risk (5%-30%), and low-risk (<5%) groups. The lymph node (LN) level was determined according to the Radiation Therapy Oncology Group guidelines, which were further categorized into the upper neck (retropharyngeal region and level II), middle neck (levels III and Va), and lower neck (levels IV and Vb and the supraclavicular fossa). The high-risk anatomic sites were adjacent to the nasopharynx, whereas those at medium-or low-risk were separated from the nasopharynx. If the high-risk anatomic sites were involved, the rates of tumor invasion into the adjacent medium-risk sites increased; if not, the rates were significantly lower (P<0.01). Among the 1920 (81.1%) patients with positive LN, the incidence rates of LN metastasis in the upper, middle, and lower neck were 99.6%, 30.2%, and 7.2%, respectively, and skip metastasis happened in only 1.2% of patients. In the 929 patients who had unilateral upper neck involvement, the rates of contralateral middle neck and lower neck involvement were 1.8% and 0.4%, respectively. Thus, local disease spreads stepwise from proximal sites to distal sites, and LN metastasis spreads from the upper neck to the lower neck. Individualized CTV delineation for NPC may be feasible.
Figures
References
-
- Parkin DM, Whelan SL, Ferlay J, et al. Vol. VIII Lyon: IARC Press; 2002. Cancer incidence in five continents.
-
- Lee N, Xia P, Quivey JM, et al. Intensity-modulated radiotherapy in the treatment of nasopharyngeal carcinoma: an update of the UCSF experience. Int J Radiat Oncol Biol Phys. 2002;53:12–22. - PubMed
-
- Kam MK, Teo PM, Chau RM, et al. Treatment of nasopharyngeal carcinoma with intensity-modulated radiotherapy: the Hong Kong experience. Int J Radiat Oncol Biol Phys. 2004;60:1440–1450. - PubMed
-
- Tham IW, Hee SW, Yeo RM, et al. Treatment of nasopharyngeal carcinoma using intensity-modulated radiotherapy—the national cancer centre Singapore experience. Int J Radiat Oncol Biol Phys. 2009;75:1481–1486. - PubMed
-
- Lin S, Pan J, Han L, et al. Nasopharyngeal carcinoma treated with reduced-volume intensity-modulated radiation therapy: report on the 3-year outcome of a prospective series. Int J Radiat Oncol Biol Phys. 2009;75:1071–1078. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources