

Treatment use and costs among privately insured youths with diagnoses of bipolar disorder
- PMID: 22855210
- PMCID: PMC4041154
- DOI: 10.1176/appi.ps.201100516
Treatment use and costs among privately insured youths with diagnoses of bipolar disorder
Abstract
Objective: Recent evidence suggests that children are increasingly diagnosed as having bipolar disorder, yet no studies have quantified treatment costs for pediatric patients. The objectives of the study were to identify one-year health services utilization and treatment costs among youths newly diagnosed as having bipolar disorder.
Methods: MarketScan administrative claims from 2005 to 2007 were used to construct a retrospective person-level cohort of children ages zero to 17 to identify one-year health services utilization and costs among privately insured youths with a bipolar diagnosis. Inpatient and outpatient services were categorized as mental health related or non–mental health related. Pharmacy costs were classified as psychotropic or nonpsychotropic.
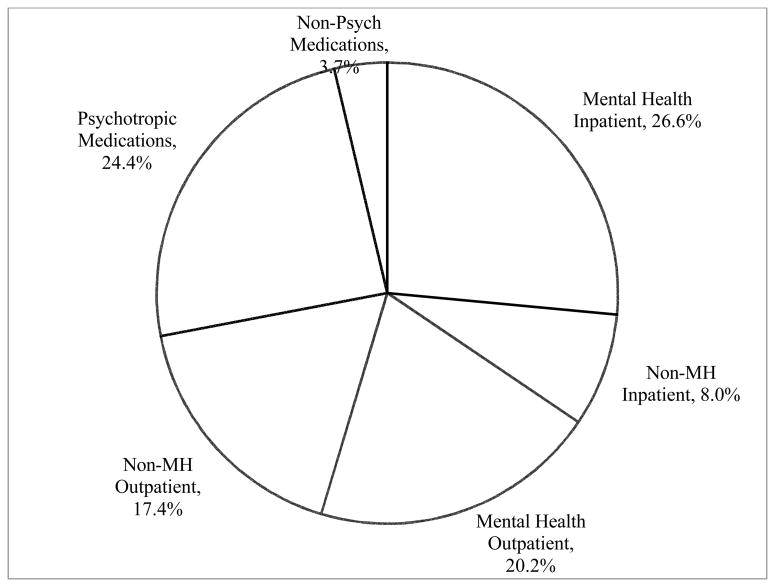
Results: In the sample (4,973 youths), one-year mean reimbursements for health services were $10,372, and patient out-of-pocket spending was $1,429 per child. Mental health services accounted for 71% of all health care spending, with psychotropic medications and inpatient care contributing the largest proportions of total spending (24% and 27%, respectively) .
Conclusions: The costs of care among privately insured children with bipolar disorder are similar to those of adults. However, spending on children is concentrated on mental health–related services. Because private insurance plans have historically limited mental health service benefits, the concentration of spending on mental health services may place a greater burden on families for out-of-pocket payments. As mental health parity is adopted by private insurers, monitoring its impact on patient utilization and costs of health services will be important, particularly for children with serious mental illness.
Conflict of interest statement
Drs. Dusetzina and Weinberger have no competing interests.
Figures
References
-
- WHO. The global burden of disease: 2004 update, Part 3: Disease incidence, prevalence and disability. Geneva, Switzerland: World Health Organization; 2008.
-
- WHO. The global burden of disease: 2004 update, Part 4: Burden of disease: DALYs. Geneva, Switzerland: World Health Organization; 2008.
-
- Costello EJ, Pine DS, Hammen C, et al. Development and natural history of mood disorders. Biological Psychiatry. 2002;52:529–542. - PubMed
-
- Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Archives of General Psychiatry. 2007;64:1032–1039. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
