

Vibration response imaging: a novel noninvasive tool for evaluating the initial therapeutic effect of noninvasive positive pressure ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease
- PMID: 22856613
- PMCID: PMC3478983
- DOI: 10.1186/1465-9921-13-65
Vibration response imaging: a novel noninvasive tool for evaluating the initial therapeutic effect of noninvasive positive pressure ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease
Abstract
Background: The popular methods for evaluating the initial therapeutic effect (ITE) of noninvasive positive pressure ventilation (NPPV) can only roughly reflect the therapeutic outcome of a patient's ventilation because they are subjective, invasive and time-delayed. In contrast, vibration response imaging (VRI) can monitor the function of a patient's ventilation over the NPPV therapy in a non-invasive manner. This study aimed to investigate the value of VRI in evaluating the ITE of NPPV for patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
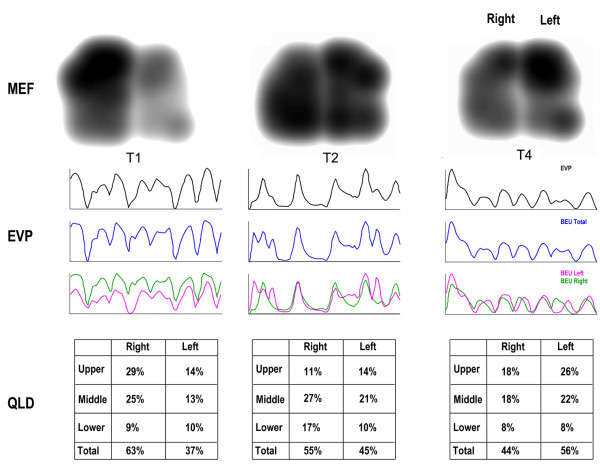
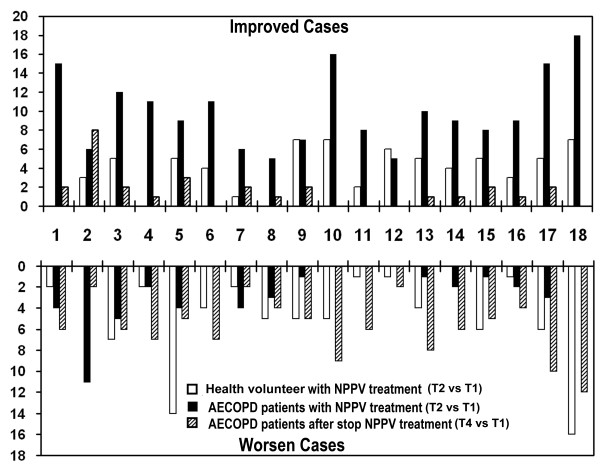
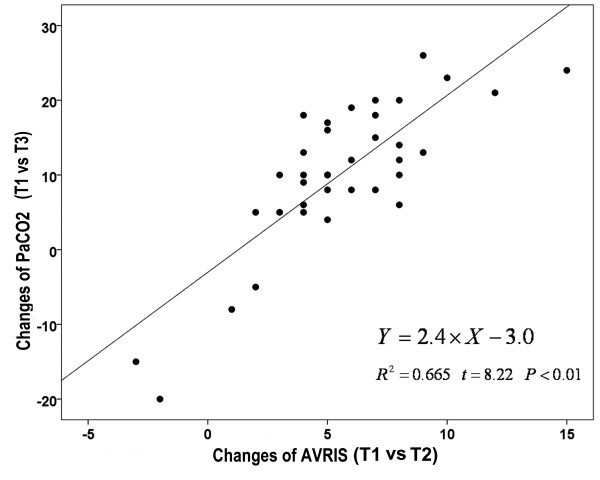
Methods: Thirty-six AECOPD patients received VRI at three time points: before NPPV treatment (T1), at 15 min of NPPV treatment (T2), and at 15 min after the end of NPPV treatment (T4). Blood gas analysis was also performed at T1 and at 2 hours of NPPV treatment (T3). Thirty-nine healthy volunteers also received VRI at T1 and T2. VRI examination at the time point T2 in either the patients or volunteers did not require any interruption of the on-going NPPV. The clinical indices at each time point were compared between the two groups. Moreover, correlations between the PaCO2 changes (T3 vs T1) and abnormal VRI scores (AVRIS) changes (T2 vs T1) were analyzed.
Results: No significant AVRIS differences were found between T1 and T2 in the healthy controls (8.51 ± 3.36 vs. 8.53 ± 3.57, P > 0.05). The AVRIS, dynamic score, MEF score and EVP score showed a significant decrease in AECOPD patients at T2 compared with T1 (P < 0.05), but a significant increase at T4 compared with T2 (P < 0.05). We also found a positive correlation (R2 = 0.6399) between the PaCO2 changes (T3 vs T1) and AVRIS changes (T2 vs T1).
Conclusions: VRI is a promising noninvasive tool for evaluating the initial therapeutic effects of NPPV in AECOPD patients and predicting the success of NPPV in the early stage.
Figures
Similar articles
-
High-intensity versus low-intensity noninvasive positive pressure ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease (HAPPEN): study protocol for a multicenter randomized controlled trial.Trials. 2018 Nov 21;19(1):645. doi: 10.1186/s13063-018-2991-y. Trials. 2018. PMID: 30463622 Free PMC article.
-
Clinical efficacy of HI-NPPV in the treatment of AECOPD combined with severe type II respiratory failure.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024 Feb 28;49(2):266-272. doi: 10.11817/j.issn.1672-7347.2024.230329. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 38755722 Free PMC article. Chinese, English.
-
Early use of noninvasive techniques for clearing respiratory secretions during noninvasive positive-pressure ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease and hypercapnic encephalopathy: A prospective cohort study.Medicine (Baltimore). 2017 Mar;96(12):e6371. doi: 10.1097/MD.0000000000006371. Medicine (Baltimore). 2017. PMID: 28328824 Free PMC article.
-
Why High-Intensity NPPV is Favourable to Low-Intensity NPPV: Clinical and Physiological Reasons.COPD. 2017 Aug;14(4):389-395. doi: 10.1080/15412555.2017.1318843. Epub 2017 May 11. COPD. 2017. PMID: 28494170 Review.
-
Nocturnal non-invasive positive pressure ventilation for COPD.Expert Rev Respir Med. 2015 Jun;9(3):295-308. doi: 10.1586/17476348.2015.1035260. Epub 2015 Apr 20. Expert Rev Respir Med. 2015. PMID: 25896807 Review.
Cited by
-
Acoustic Lung Imaging Utilized in Continual Assessment of Patients with Obstructed Airway: A Systematic Review.Sensors (Basel). 2023 Jul 7;23(13):6222. doi: 10.3390/s23136222. Sensors (Basel). 2023. PMID: 37448069 Free PMC article.
-
Evaluation of Vibration Response Imaging (VRI) Technique and Difference in VRI Indices Among Non-Smokers, Active Smokers and Passive Smokers.Med Sci Monit. 2015 Jul 27;21:2170-7. doi: 10.12659/MSM.894335. Med Sci Monit. 2015. PMID: 26212715 Free PMC article.
-
Thoracic Imaging at Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review.Int J Chron Obstruct Pulmon Dis. 2020 Jul 22;15:1751-1787. doi: 10.2147/COPD.S250746. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32801677 Free PMC article.
References
-
- Lightowler JV, Wedzicha JA, Elliott MW, Ram FS. Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003;326(7382):185. doi: 10.1136/bmj.326.7382.185. - DOI - PMC - PubMed
-
- Squadrone E, Frigerio P, Fogliati C, Gregoretti C, Conti G, Antonelli M. et al.Noninvasive vs invasive ventilation in COPD patients with severe acute respiratory failure deemed to require ventilatory assistance. Intensive Care Med. 2004;30(7):1303–1310. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
