

Impact of retrospective calibration algorithms on hypoglycemia detection in newborn infants using continuous glucose monitoring
- PMID: 22856622
- PMCID: PMC3459024
- DOI: 10.1089/dia.2012.0111
Impact of retrospective calibration algorithms on hypoglycemia detection in newborn infants using continuous glucose monitoring
Abstract
Background: Neonatal hypoglycemia is common and may cause serious brain injury. Diagnosis is by blood glucose (BG) measurements, often taken several hours apart. Continuous glucose monitoring (CGM) could improve hypoglycemia detection, while reducing the number of BG measurements. Calibration algorithms convert sensor signals into CGM output. Thus, these algorithms directly affect measures used to quantify hypoglycemia. This study was designed to quantify the effects of recalibration and filtering of CGM data on measures of hypoglycemia (BG <2.6 mmol/L) in neonates.
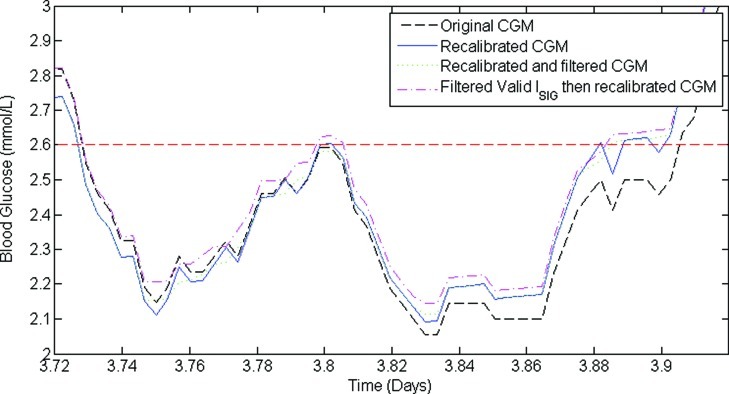
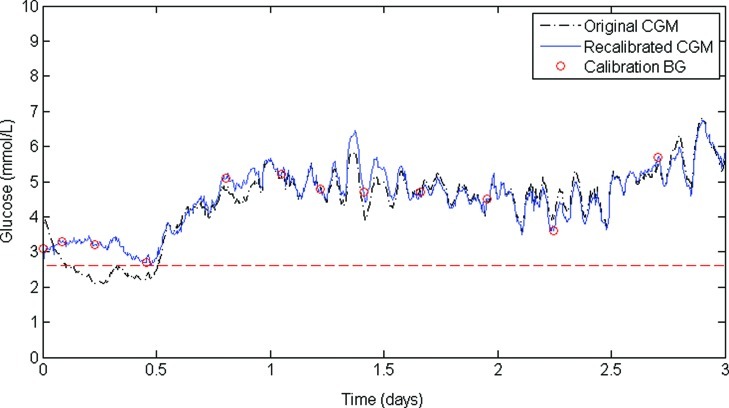
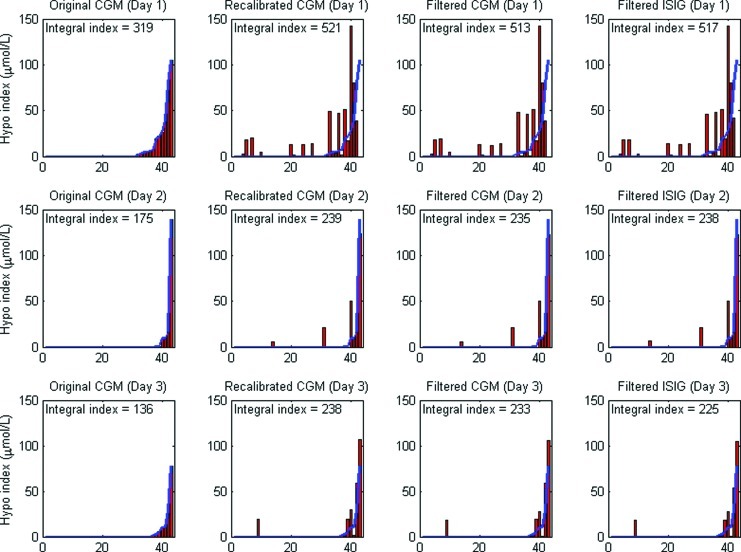
Subjects and methods: CGM data from 50 infants were recalibrated using an algorithm that explicitly recognized the high-accuracy BG measurements available in this study. CGM data were analyzed as (1) original CGM output, (2) recalibrated CGM output, (3) recalibrated CGM output with postcalibration median filtering, and (4) recalibrated CGM output with precalibration median filtering. Hypoglycemia was classified by number of episodes, duration, severity, and hypoglycemic index.
Results: Recalibration increased the number of hypoglycemic events (from 161 to 193), hypoglycemia duration (from 2.2% to 2.6%), and hypoglycemic index (from 4.9 to 7.1 μmol/L). Median filtering postrecalibration reduced hypoglycemic events from 193 to 131, with little change in duration (from 2.6% to 2.5%) and hypoglycemic index (from 7.1 to 6.9 μmol/L). Median filtering prerecalibration resulted in 146 hypoglycemic events, a total duration of hypoglycemia of 2.6%, and a hypoglycemic index of 6.8 μmol/L.
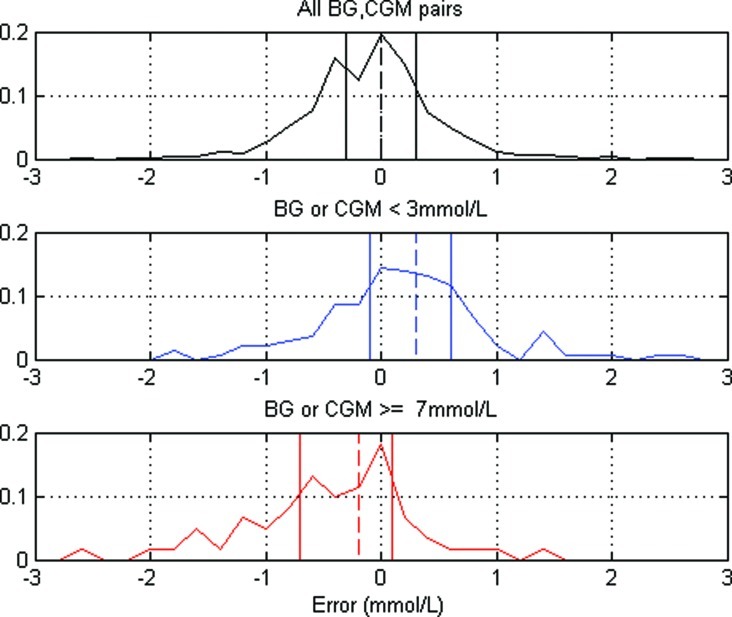
Conclusions: Hypoglycemia metrics, especially counting events, are heavily dependent on CGM calibration BG error, and the calibration algorithm. CGM devices tended to read high at lower levels, so when high accuracy calibration measurements are available it may be more appropriate to recalibrate the data.
Figures
Similar articles
-
Continuous glucose monitoring in newborn infants: how do errors in calibration measurements affect detected hypoglycemia?J Diabetes Sci Technol. 2014 May;8(3):543-50. doi: 10.1177/1932296814524857. Epub 2014 Feb 27. J Diabetes Sci Technol. 2014. PMID: 24876618 Free PMC article.
-
Accuracy evaluation of a new real-time continuous glucose monitoring algorithm in hypoglycemia.Diabetes Technol Ther. 2014 Oct;16(10):667-78. doi: 10.1089/dia.2014.0043. Epub 2014 Jun 11. Diabetes Technol Ther. 2014. PMID: 24918271
-
Accuracy of a new real-time continuous glucose monitoring algorithm.J Diabetes Sci Technol. 2010 Jan 1;4(1):111-8. doi: 10.1177/193229681000400114. J Diabetes Sci Technol. 2010. PMID: 20167174 Free PMC article.
-
Reduction of number and duration of hypoglycemic events by glucose prediction methods: a proof-of-concept in silico study.Diabetes Technol Ther. 2013 Jan;15(1):66-77. doi: 10.1089/dia.2012.0208. Diabetes Technol Ther. 2013. PMID: 23297671 Review.
-
Neonatal hypoglycemia: continuous glucose monitoring.Curr Opin Pediatr. 2018 Apr;30(2):204-208. doi: 10.1097/MOP.0000000000000592. Curr Opin Pediatr. 2018. PMID: 29346140 Free PMC article. Review.
Cited by
-
Continuous glucose monitoring in neonates: a review.Matern Health Neonatol Perinatol. 2017 Oct 17;3:18. doi: 10.1186/s40748-017-0055-z. eCollection 2017. Matern Health Neonatol Perinatol. 2017. PMID: 29051825 Free PMC article. Review.
-
Association of Neonatal Hypoglycemia With Academic Performance in Mid-Childhood.JAMA. 2022 Mar 22;327(12):1158-1170. doi: 10.1001/jama.2022.0992. JAMA. 2022. PMID: 35315886 Free PMC article.
-
Comparison between one-point calibration and two-point calibration approaches in a continuous glucose monitoring algorithm.J Diabetes Sci Technol. 2014 Jul;8(4):709-19. doi: 10.1177/1932296814531356. Epub 2014 Apr 21. J Diabetes Sci Technol. 2014. PMID: 24876420 Free PMC article.
-
Stability of executive function in children born at risk of neonatal hypoglycemia.Child Neuropsychol. 2023 Nov 27:1-20. doi: 10.1080/09297049.2023.2285391. Online ahead of print. Child Neuropsychol. 2023. PMID: 38010710 Free PMC article.
-
Neonatal Glycemia and Neurodevelopmental Outcomes at 2 Years.N Engl J Med. 2015 Oct 15;373(16):1507-18. doi: 10.1056/NEJMoa1504909. N Engl J Med. 2015. PMID: 26465984 Free PMC article.
References
-
- Stanley CA. Baker L. The causes of neonatal hypoglycemia. N Engl J Med. 1999;340:1200–1201. - PubMed
-
- Cornblath M. Hawdon JM. Williams AF. Aynsley-Green A. Ward-Platt MP. Schwartz R. Kalhan SC. Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds. Pediatrics. 2000;105:1141–1145. - PubMed
-
- Harris DL. Battin MR. Weston PJ. Harding JE. Continuous glucose monitoring in newborn babies at risk of hypoglycemia. J Pediatr. 2010;157:198–202. - PubMed
-
- Klonoff DC. The importance of continuous glucose monitoring in diabetes. Diabetes Technol Ther. 2000;2(Suppl 1):S1–S3.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
