

Diagnostic and prognostic value of cardiovascular magnetic resonance in non-ischaemic cardiomyopathies
- PMID: 22857649
- PMCID: PMC3436728
- DOI: 10.1186/1532-429X-14-54
Diagnostic and prognostic value of cardiovascular magnetic resonance in non-ischaemic cardiomyopathies
Abstract
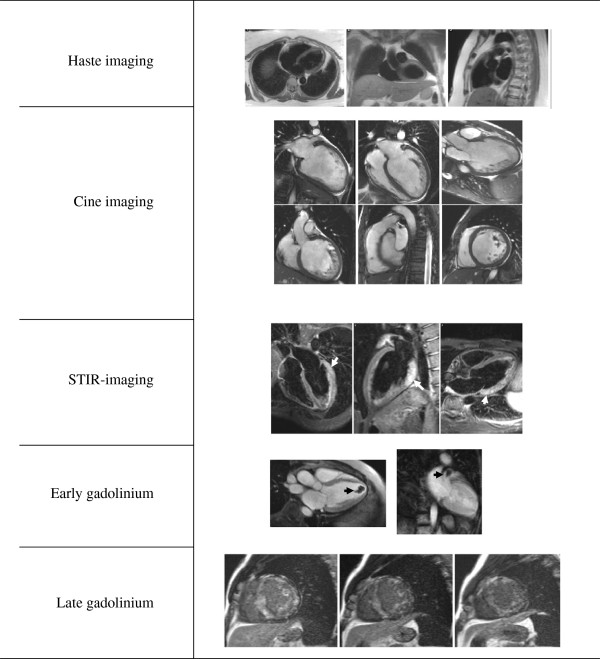
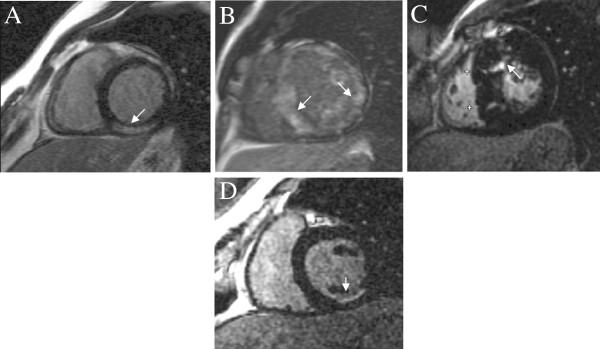
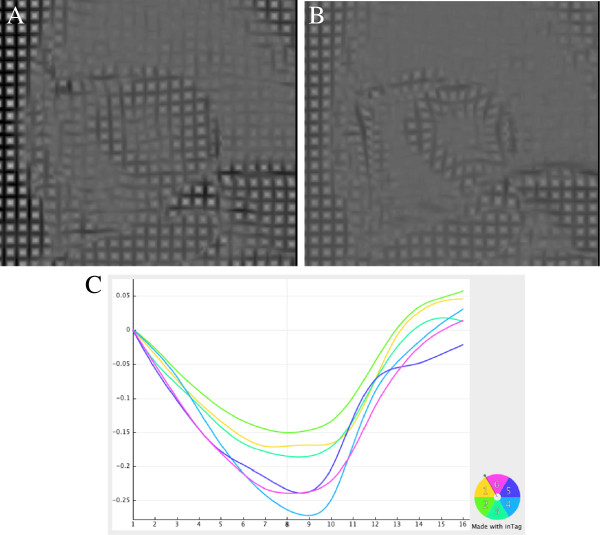
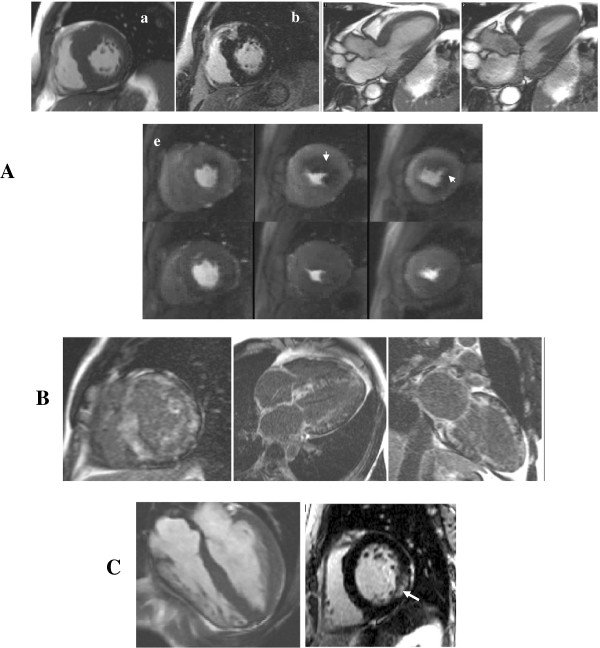
Cardiovascular Magnetic Resonance (CMR) is recognised as a valuable clinical tool which in a single scan setting can assess ventricular volumes and function, myocardial fibrosis, iron loading, flow quantification, tissue characterisation and myocardial perfusion imaging. The advent of CMR using extrinsic and intrinsic contrast-enhanced protocols for tissue characterisation have dramatically changed the non-invasive work-up of patients with suspected or known cardiomyopathy. Although the technique initially focused on the in vivo identification of myocardial necrosis through the late gadolinium enhancement (LGE) technique, recent work highlighted the ability of CMR to provide more detailed in vivo tissue characterisation to help establish a differential diagnosis of the underlying aetiology, to exclude an ischaemic substrate and to provide important prognostic markers. The potential application of CMR in the clinical approach of a patient with suspected non-ischaemic cardiomyopathy is discussed in this review.
Figures
References
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. doi: 10.1161/CIRCULATIONAHA.106.174287. - DOI - PubMed
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, Dubourg O, Kuhl U, Maisch B, McKenna WJ. et al.Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–276. - PubMed
-
- Assomull RG, Shakespeare C, Kalra PR, Lloyd G, Gulati A, Strange J, Bradlow WM, Lyne J, Keegan J, Poole-Wilson P. et al.Role of Cardiovascular Magnetic Resonance as a Gatekeeper to Invasive Coronary Angiography in Patients Presenting With Heart Failure of Unknown Etiology. Circulation. 2011;124:1351–1360. doi: 10.1161/CIRCULATIONAHA.110.011346. - DOI - PubMed
-
- Kramer CM, Barkhausen J, Flamm SD, Kim RJ, Nagel E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols, society for cardiovascular magnetic resonance: board of trustees task force on standardized protocols. Journal of Cardiovascular Magnetic Resonance. 2008;10:35. doi: 10.1186/1532-429X-10-35. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
