

Restenosis after carotid artery stenting and endarterectomy: a secondary analysis of CREST, a randomised controlled trial
- PMID: 22857850
- PMCID: PMC3912998
- DOI: 10.1016/S1474-4422(12)70159-X
Restenosis after carotid artery stenting and endarterectomy: a secondary analysis of CREST, a randomised controlled trial
Abstract
Background: In the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), the composite primary endpoint of stroke, myocardial infarction, or death during the periprocedural period or ipsilateral stroke thereafter did not differ between carotid artery stenting and carotid endarterectomy for symptomatic or asymptomatic carotid stenosis. A secondary aim of this randomised trial was to compare the composite endpoint of restenosis or occlusion.
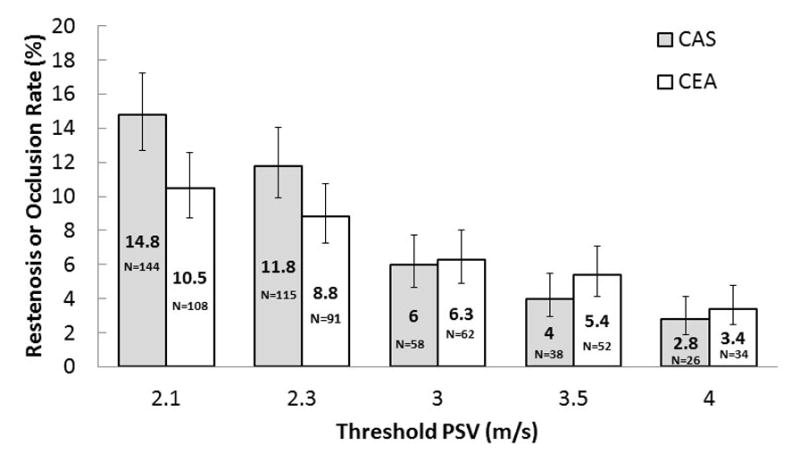
Methods: Patients with stenosis of the carotid artery who were asymptomatic or had had a transient ischaemic attack, amaurosis fugax, or a minor stroke were eligible for CREST and were enrolled at 117 clinical centres in the USA and Canada between Dec 21, 2000, and July 18, 2008. In this secondary analysis, the main endpoint was a composite of restenosis or occlusion at 2 years. Restenosis and occlusion were assessed by duplex ultrasonography at 1, 6, 12, 24, and 48 months and were defined as a reduction in diameter of the target artery of at least 70%, diagnosed by a peak systolic velocity of at least 3·0 m/s. Studies were done in CREST-certified laboratories and interpreted at the Ultrasound Core Laboratory (University of Washington). The frequency of restenosis was calculated by Kaplan-Meier survival estimates and was compared during a 2-year follow-up period. We used proportional hazards models to assess the association between baseline characteristics and risk of restenosis. Analyses were per protocol. CREST is registered with ClinicalTrials.gov, number NCT00004732.
Findings: 2191 patients received their assigned treatment within 30 days of randomisation and had eligible ultrasonography (1086 who had carotid artery stenting, 1105 who had carotid endarterectomy). In 2 years, 58 patients who underwent carotid artery stenting (Kaplan-Meier rate 6·0%) and 62 who had carotid endarterectomy (6·3%) had restenosis or occlusion (hazard ratio [HR] 0·90, 95% CI 0·63-1·29; p=0·58). Female sex (1·79, 1·25-2·56), diabetes (2·31, 1·61-3·31), and dyslipidaemia (2·07, 1·01-4·26) were independent predictors of restenosis or occlusion after the two procedures. Smoking predicted an increased rate of restenosis after carotid endarterectomy (2·26, 1·34-3·77) but not after carotid artery stenting (0·77, 0·41-1·42).
Interpretation: Restenosis and occlusion were infrequent and rates were similar up to 2 years after carotid endarterectomy and carotid artery stenting. Subsets of patients could benefit from early and frequent monitoring after revascularisation.
Funding: National Institute of Neurological Disorders and Stroke and Abbott Vascular Solutions.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures

Comment in
-
Restenosis after carotid artery stenting: remaining issues.Lancet Neurol. 2012 Sep;11(9):740-1. doi: 10.1016/S1474-4422(12)70179-5. Epub 2012 Aug 2. Lancet Neurol. 2012. PMID: 22857849 No abstract available.
-
Restenosis after carotid endarterectomy and stenting--authors' reply.Lancet Neurol. 2013 Feb;12(2):130-1. doi: 10.1016/S1474-4422(12)70260-0. Epub 2012 Nov 12. Lancet Neurol. 2013. PMID: 23151439 No abstract available.
-
Restenosis after carotid endarterectomy and stenting.Lancet Neurol. 2013 Feb;12(2):130. doi: 10.1016/S1474-4422(12)70261-2. Epub 2012 Nov 12. Lancet Neurol. 2013. PMID: 23151440 No abstract available.
References
-
- Lal BK, Hobson RWII, Goldstein J, et al. In-stent recurrent stenosis after carotid artery stenting: life table analysis and clinical relevance. J Vasc Surg. 2003;38:1162–8. discussion 1169. - PubMed
-
- Bonati LH, Ederle J, McCabe DJH, et al. Long-term risk of carotid restenosis in patients randomly assigned to endovascular treatment or endarterectomy in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): long-term follow-up of a randomised trial. Lancet Neurol. 2009;8:908–17. - PMC - PubMed
-
- Eckstein H-H, Ringleb P, Allenberg J-R, et al. Results of the Stent-protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol. 2008;7:893–902. - PubMed
-
- Arquizan C, Trinquart L, Touboul P-J, et al. Restenosis is more frequent after carotid stenting than after endarterectomy. Stroke. 2011;42:1015–20. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
