

Evaluating CT perfusion using outcome measures of delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage
- PMID: 22859289
- PMCID: PMC4004022
- DOI: 10.3174/ajnr.A3225
Evaluating CT perfusion using outcome measures of delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage
Abstract
Background and purpose: DCI is a serious complication following aneurysmal SAH and remains a leading cause of morbidity and mortality. Our aim was to evaluate CTP in aneurysmal SAH by using outcome measures of DCI.
Materials and methods: This was a retrospective study of consecutive patients with SAH enrolled in a prospective institutional review board-approved clinical accuracy trial. Qualitative CTP deficits were determined by 2 neuroradiologists blinded to clinical and imaging data. Quantitative CTP was performed by using a standardized protocol with region-of-interest placement sampling of the cortex. Primary outcome measures were permanent neurologic deficits and infarction. The secondary outcome measure was DCI, defined as clinical deterioration. CTP test characteristics (95% CI) were determined for each outcome measure. Statistical significance was calculated by using the Fisher exact and Student t tests. ROC curves were generated to determine accuracy and threshold analysis.
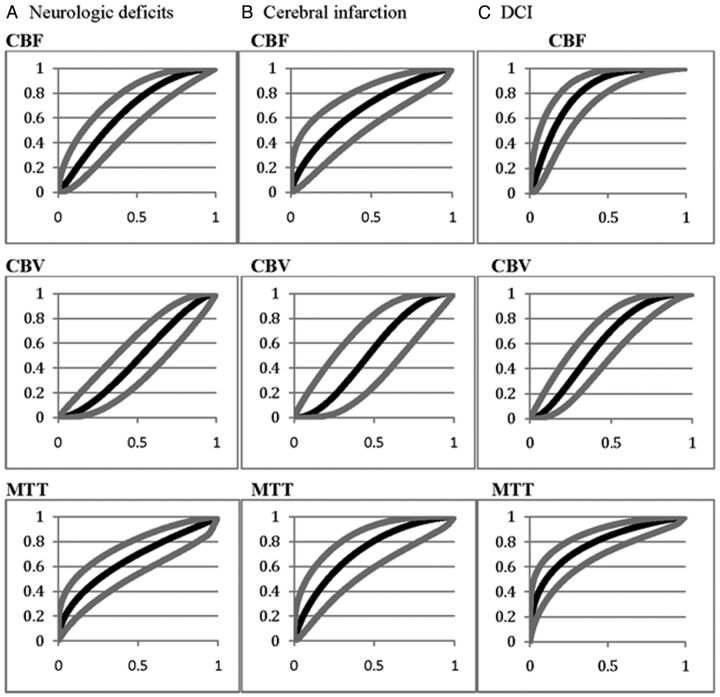
Results: Ninety-six patients were included. Permanent neurologic deficits developed in 33% (32/96). CTP deficits were seen in 78% (25/32) of those who developed permanent neurologic deficits and 34% (22/64) of those without (P < .0001). CTP deficits had 78% (61%-89%) sensitivity, 66% (53%-76%) specificity, and 53% (39%-67%) positive and 86% (73%-93%) negative predictive values. Infarction occurred in 18% (17/96). CTP deficits were seen in 88% (15/17) of those who developed infarction and 41% (32/79) of those without (P = .0004). CTP deficits had an 88% (66%-97%) sensitivity, 59% (48%-70%) specificity, and 32% (20%-46%) positive and 96% (86%-99%) negative predictive values. DCI was diagnosed in 50% (48/96). CTP deficits were seen in 81% (39/48) of patients with DCI and in 17% (8/48) of those without (P < .0001). CTP deficits had 81% (68%-90%) sensitivity, 83% (70%-91%) specificity, and 83% (70%-91%) positive and 82% (69%-90%) negative predictive values. Quantitative CTP revealed significantly reduced CBF and prolonged MTT for DCI, permanent neurologic deficits, and infarction. ROC analysis showed that CBF and MTT had the highest accuracy.
Conclusions: CTP may add prognostic information regarding DCI and poor outcomes in aneurysmal SAH.
Figures
References
-
- Vergouwen MD, Vermeulen M, van Gijn J, et al. . Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke 2010;41:2391–95 - PubMed
-
- Dankbaar JW, de Rooij NK, Velthuis BK, et al. . Diagnosing delayed cerebral ischemia with different CT modalities in patients with subarachnoid hemorrhage with clinical deterioration. Stroke 2009;40:3493–98 - PubMed
-
- Dankbaar JW, de Rooij NK, Rijsdijk M, et al. . Diagnostic threshold values of cerebral perfusion measured with computed tomography for delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Stroke 2010;41:1927–32 - PubMed
-
- Aralasmak A, Akyuz M, Ozkaynak C, et al. . CT angiography and perfusion imaging in patients with subarachnoid hemorrhage: correlation of vasospasm to perfusion abnormality. Neuroradiology 2009;51:85–93 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical