

STAT3 mutations unify the pathogenesis of chronic lymphoproliferative disorders of NK cells and T-cell large granular lymphocyte leukemia
- PMID: 22859607
- PMCID: PMC3471515
- DOI: 10.1182/blood-2012-06-435297
STAT3 mutations unify the pathogenesis of chronic lymphoproliferative disorders of NK cells and T-cell large granular lymphocyte leukemia
Abstract
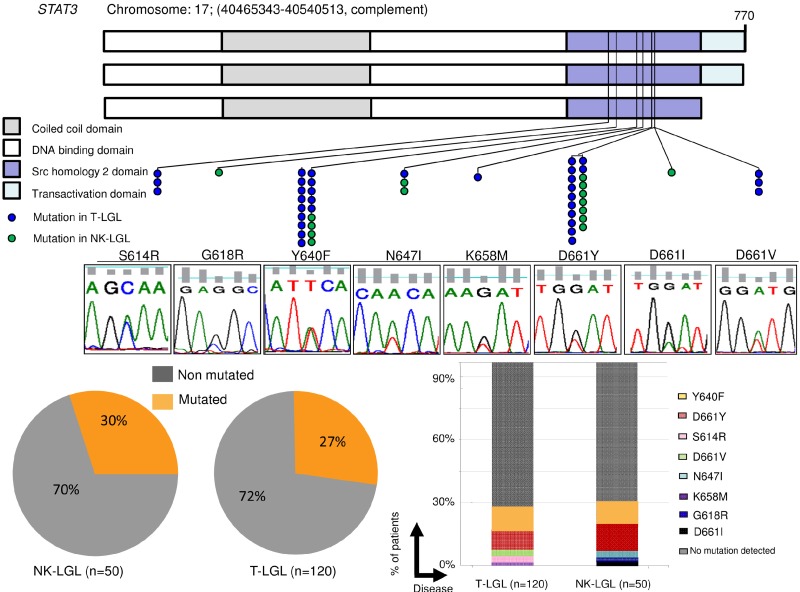
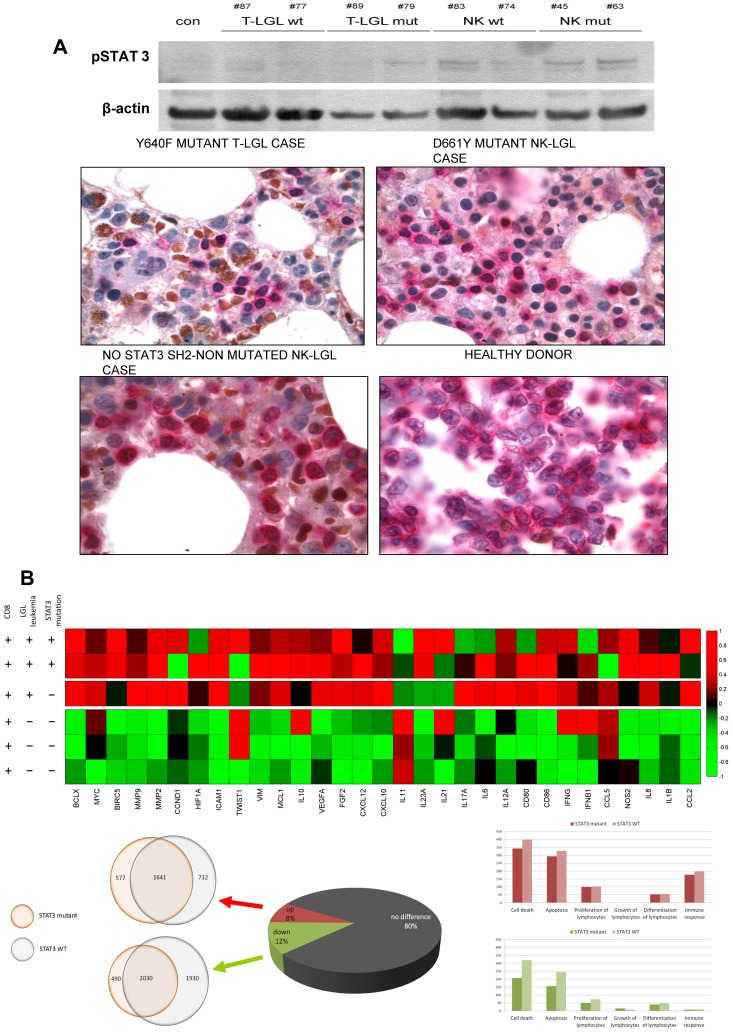
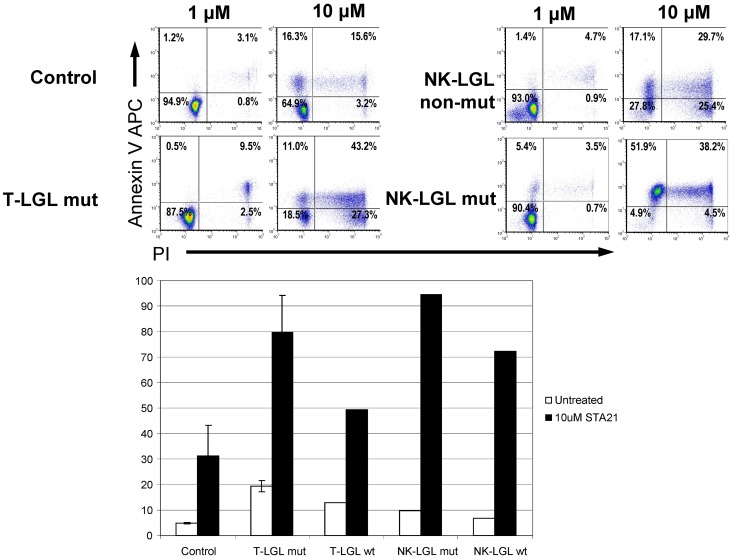
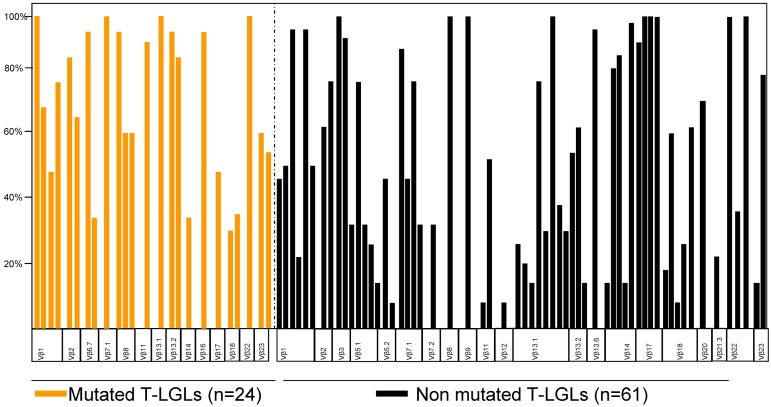
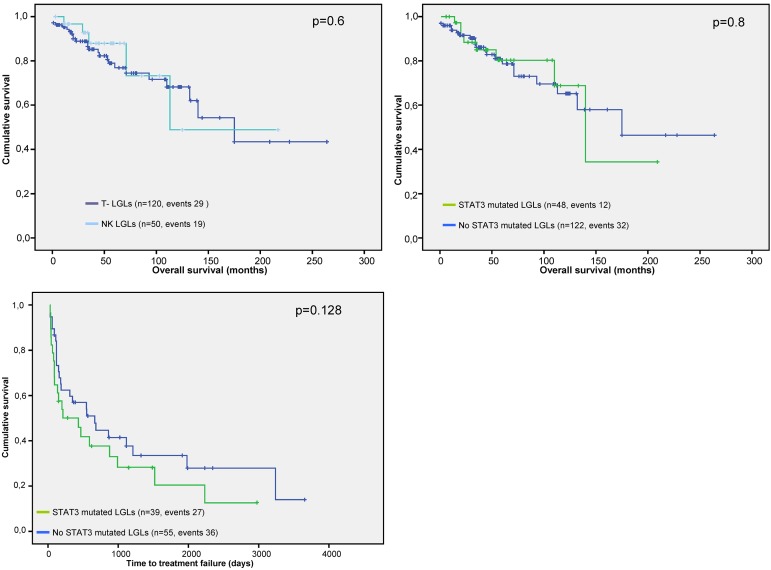
Chronic lymphoproliferative disorders of natural killer cells (CLPD-NKs) and T-cell large granular lymphocytic leukemias (T-LGLs) are clonal lymphoproliferations arising from either natural killer cells or cytotoxic T lymphocytes (CTLs). We have investigated for distribution and functional significance of mutations in 50 CLPD-NKs and 120 T-LGL patients by direct sequencing, allele-specific PCR, and microarray analysis. STAT3 gene mutations are present in both T and NK diseases: approximately one-third of patients with each type of disorder convey these mutations. Mutations were found in exons 21 and 20, encoding the Src homology 2 domain. Patients with mutations are characterized by symptomatic disease (75%), history of multiple treatments, and a specific pattern of STAT3 activation and gene deregulation, including increased expression of genes activated by STAT3. Many of these features are also found in patients with wild-type STAT3, indicating that other mechanisms of STAT3 activation can be operative in these chronic lymphoproliferative disorders. Treatment with STAT3 inhibitors, both in wild-type and mutant cases, resulted in accelerated apoptosis. STAT3 mutations are frequent in large granular lymphocytes suggesting a similar molecular dysregulation in malignant chronic expansions of NK and CTL origin. STAT3 mutations may distinguish truly malignant lymphoproliferations involving T and NK cells from reactive expansions.
Figures
References
-
- Loughran TP, Jr, Kadin ME, Starkebaum G, et al. Leukemia of large granular lymphocytes: association with clonal chromosomal abnormalities and autoimmune neutropenia, thrombocytopenia, and hemolytic anemia. Ann Intern Med. 1985;102(2):169–175. - PubMed
-
- Loughran TP., Jr Clonal diseases of large granular lymphocytes. Blood. 1993;82(1):1–14. - PubMed
-
- Swerdlow SH. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th Ed. Lyon, France: International Agency for Research on Cancer; 2008. International Agency for Research on Cancer, World Health Organization.
-
- Swerdlow SH, Harris NL, editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th Ed. Lyon, France: International Agency for Research on Cancer; 2008.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
