

Diagnostic biopsy does not commonly induce intratumoral CD8 T cell infiltration in Merkel cell carcinoma
- PMID: 22859987
- PMCID: PMC3409202
- DOI: 10.1371/journal.pone.0041465
Diagnostic biopsy does not commonly induce intratumoral CD8 T cell infiltration in Merkel cell carcinoma
Erratum in
- PLoS One. 2012;7(10). doi: 10.1371/annotation/c4df91b0-618f-464d-a613-d99758de3f3d
Abstract
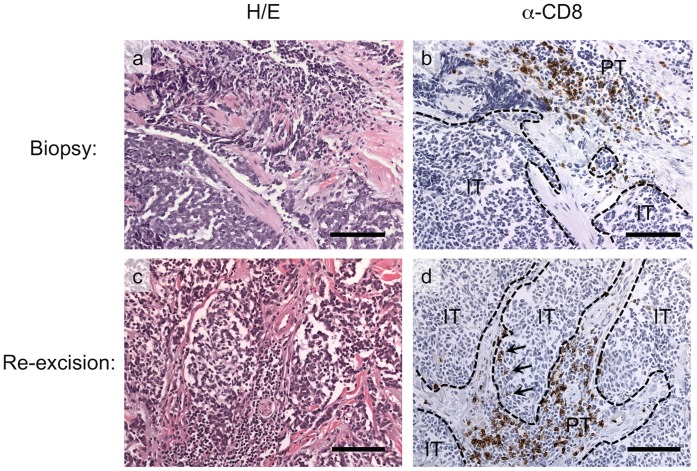
Background: Merkel cell carcinoma is a polyomavirus-associated cancer that is strongly linked with T lymphocyte immune suppression in epidemiologic studies. CD8+ T cell infiltration into MCC tumors (intratumoral) has recently been shown to be strongly predictive of improved survival. In contrast, the presence of CD8+ T cells at the border of the tumor (peritumoral) had no independent prognostic value. Spontaneous regression has been reported for MCC approximately one thousand times more often than would be expected given the frequency of this cancer. Many of these events began shortly after biopsy, and in some cases lymphocytic infiltration was described.
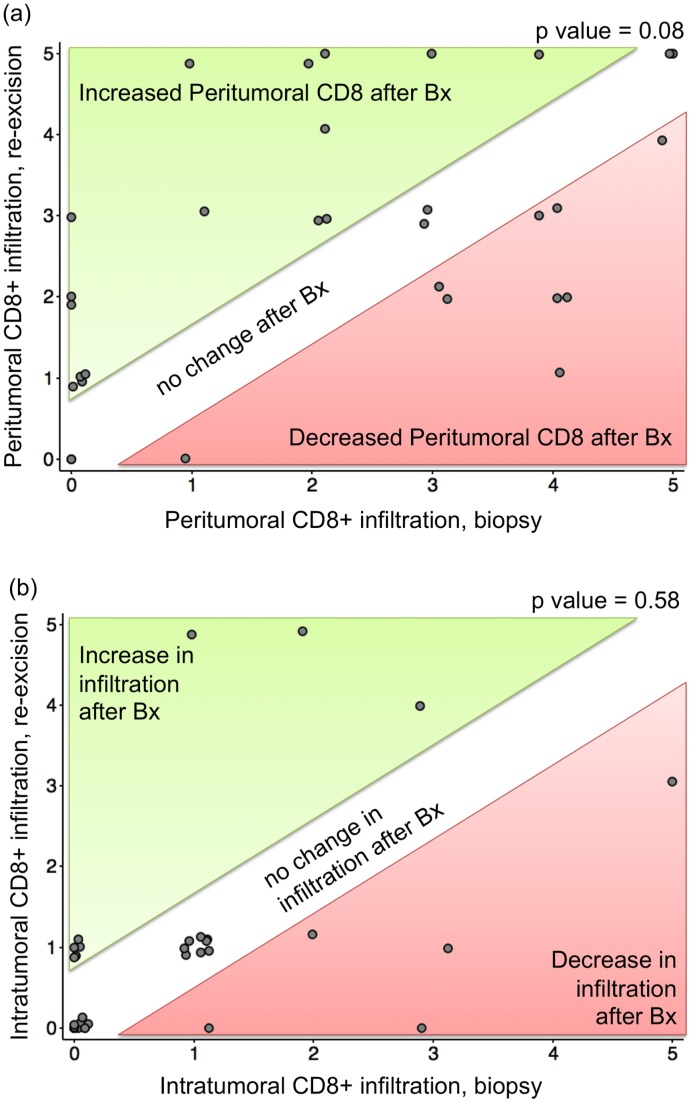
Methodology/principal findings: To determine whether CD8+ lymphocyte infiltration in MCC tumors is commonly altered by biopsy.33 MCC patients who had microscopic confirmation of MCC on both an initial biopsy and a re-excision specimen were included in this study. Intratumoral and peritumoral CD8 lymphocyte infiltration was quantitated using immunohistochemistry and compared using the paired t-test in biopsy versus re-excision samples. There was a trend toward increased CD8 infiltration after biopsy in a peritumoral ('stalled') pattern (p = 0.08), however, biopsy was not associated with a significant increase in CD8 T cells in the clinically more important intratumoral location (p = 0.58).
Conclusions/significance: The initial diagnostic biopsy for MCC does not commonly alter intratumoral CD8+ T cell infiltration, suggesting it does not directly induce immunologic recognition of this cancer. Because CD8 infiltration is typically stable after biopsy, this parameter may be useful to assess the efficacy of future immune therapies for this virus-associated, immunogenic, often-lethal cancer.
Conflict of interest statement
Figures
Similar articles
-
Transcriptome-wide studies of merkel cell carcinoma and validation of intratumoral CD8+ lymphocyte invasion as an independent predictor of survival.J Clin Oncol. 2011 Apr 20;29(12):1539-46. doi: 10.1200/JCO.2010.30.6308. Epub 2011 Mar 21. J Clin Oncol. 2011. PMID: 21422430 Free PMC article.
-
Vascular E-selectin expression correlates with CD8 lymphocyte infiltration and improved outcome in Merkel cell carcinoma.J Invest Dermatol. 2013 Aug;133(8):2065-73. doi: 10.1038/jid.2013.36. Epub 2013 Jan 25. J Invest Dermatol. 2013. PMID: 23353989 Free PMC article.
-
CD8+ lymphocyte intratumoral infiltration as a stage-independent predictor of Merkel cell carcinoma survival: a population-based study.Am J Clin Pathol. 2014 Oct;142(4):452-8. doi: 10.1309/AJCPIKDZM39CRPNC. Am J Clin Pathol. 2014. PMID: 25239411 Free PMC article.
-
Complete spontaneous regression of primary Merkel cell carcinoma with tumoural infiltration: a systematic review.Eur J Dermatol. 2021 Jun 1;31(3):381-391. doi: 10.1684/ejd.2021.4065. Eur J Dermatol. 2021. PMID: 34080974
-
Complete Spontaneous Regression of Merkel Cell Carcinoma After Biopsy: A Case Report and Review of the Literature.Am J Dermatopathol. 2016 Nov;38(11):e154-e158. doi: 10.1097/DAD.0000000000000614. Am J Dermatopathol. 2016. PMID: 27759689 Review.
Cited by
-
Spontaneous Regression of Merkel Cell Carcinoma: Case Report.Int Med Case Rep J. 2021 Oct 2;14:711-717. doi: 10.2147/IMCRJ.S329545. eCollection 2021. Int Med Case Rep J. 2021. PMID: 34629908 Free PMC article.
-
Merkel cell carcinoma of the head and neck: pathogenesis, current and emerging treatment options.Onco Targets Ther. 2015 Aug 19;8:2157-67. doi: 10.2147/OTT.S72202. eCollection 2015. Onco Targets Ther. 2015. PMID: 26316785 Free PMC article. Review.
-
The role of the immune response in merkel cell carcinoma.Cancers (Basel). 2013 Feb 28;5(1):234-54. doi: 10.3390/cancers5010234. Cancers (Basel). 2013. PMID: 24216706 Free PMC article.
-
Spontaneous Regression of Primitive Merkel Cell Carcinoma.Rare Tumors. 2015 Dec 29;7(4):5961. doi: 10.4081/rt.2015.5961. eCollection 2015 Dec 29. Rare Tumors. 2015. PMID: 26788270 Free PMC article.
-
A Spontaneous Regression of an Isolated Lymph Node Metastasis from a Primary Unknown Merkel Cell Carcinoma in a Patient with an Idiopathic Hyper-Eosinophilic Syndrome.Am J Case Rep. 2018 Dec 4;19:1437-1440. doi: 10.12659/AJCR.911840. Am J Case Rep. 2018. PMID: 30510152 Free PMC article.
References
-
- Hodgson NC (2005) Merkel cell carcinoma: changing incidence trends. J Surg Oncol 89: 1–4. - PubMed
-
- Lemos B, Nghiem P (2007) Merkel cell carcinoma: more deaths but still no pathway to blame. J Invest Dermatol 127: 2100–2103. - PubMed
-
- Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, et al. (2001) Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol 19: 3622–3634. - PubMed
Publication types
MeSH terms
Grants and funding
- RC2 CA147820/CA/NCI NIH HHS/United States
- K24 CA139052/CA/NCI NIH HHS/United States
- ULRR025014/PHS HHS/United States
- F30 ES017385/ES/NIEHS NIH HHS/United States
- TL1 RR025016/RR/NCRR NIH HHS/United States
- NIH T32CA80416-10/CA/NCI NIH HHS/United States
- TL1RR025016/RR/NCRR NIH HHS/United States
- T32 CA080416/CA/NCI NIH HHS/United States
- P30 CA015704/CA/NCI NIH HHS/United States
- NIH K24 CA139052-0/CA/NCI NIH HHS/United States
- NIH RC2CA147820/CA/NCI NIH HHS/United States
- F30ES017385/ES/NIEHS NIH HHS/United States
- TL1 TR000422/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
