

Beneficial effects on arterial stiffness and pulse-wave reflection of combined enalapril and candesartan in chronic kidney disease--a randomized trial
- PMID: 22860014
- PMCID: PMC3409235
- DOI: 10.1371/journal.pone.0041757
Beneficial effects on arterial stiffness and pulse-wave reflection of combined enalapril and candesartan in chronic kidney disease--a randomized trial
Abstract
Background: Cardiovascular disease (CVD) is highly prevalent in patients with chronic kidney disease (CKD). Inhibition of the renin-angiotensinsystem (RAS) in hypertension causes differential effects on central and brachial blood pressure (BP), which has been translated into improved outcome. The objective was to examine if a more complete inhibition of RAS by combining an angiotensin converting enzyme inhibitor (ACEI) and an angiotensin receptor antagonist (ARB) compared to monotherapy has an additive effect on central BP and pulse-wave velocity (PWV), which are known markers of CVD.
Methods: Sixty-seven CKD patients (mean GFR 30, range 13-59 ml/min/1.73 m(2)) participated in an open randomized study of 16 weeks of monotherapy with either enalapril or candesartan followed by 8 weeks of dual blockade aiming at a total dose of 16 mg candesartan and 20 mg enalapril o.d. Pulse-wave measurements were performed at week 0, 8, 16 and 24 by the SphygmoCor device.
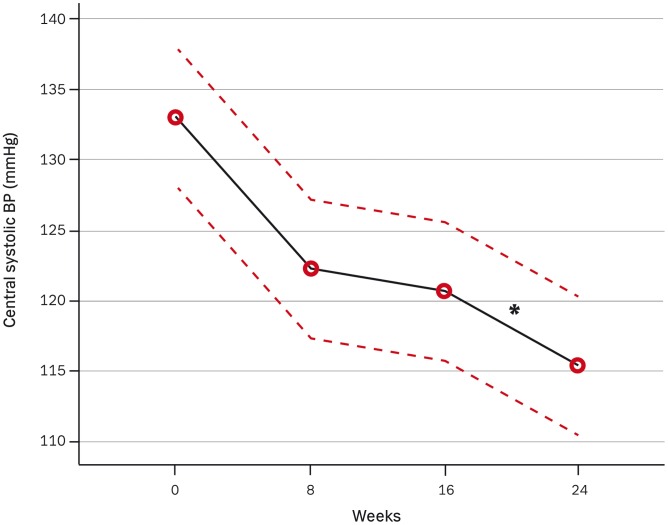
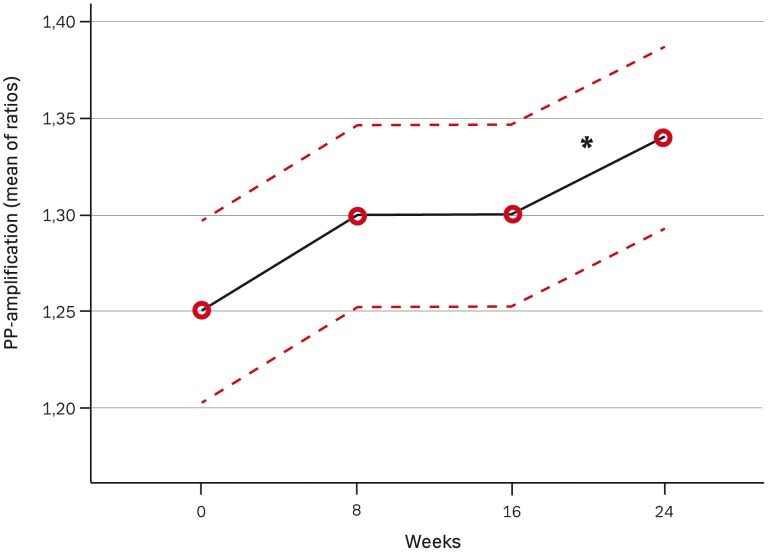
Results: Significant additive BP independent reductions were found after dual blockade in aortic PWV (-0.3 m/s, P<0.05) and in augmentation index (-2%, P<0.01) compared to monotherapy. Furthermore pulse pressure amplification was improved (P<0.05) and central systolic BP reduced (-6 mmHg, P<0.01).
Conclusions: Dual blockade of the RAS resulted in an additive BP independent reduction in pulse-wave reflection and arterial stiffness compared to monotherapy in CKD patients.
Trial registration: Clinical trial.gov NCT00235287.
Conflict of interest statement
Figures


References
-
- Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, et al. (1999) Impact of aortic stiffness on survival in end-stage renal disease. Circulation 99: 2434–2439. - PubMed
-
- London GM, Blacher J, Pannier B, Guerin AP, Marchais SJ, et al. (2001) Arterial wave reflections and survival in end-stage renal failure. Hypertension 38: 434–438. - PubMed
-
- Covic A, Haydar AA, Bhamra-Ariza P, Gusbeth-Tatomir P, Goldsmith DJ (2005) Aortic pulse wave velocity and arterial wave reflections predict the extent and severity of coronary artery disease in chronic kidney disease patients. J Nephrol 18: 388–396. - PubMed
-
- Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, et al. (2000) Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med 342: 145–153. - PubMed
-
- Brenner BM, Cooper ME, de ZD, Keane WF, Mitch WE, et al. (2001) Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
