

A pilot randomized controlled trial of a decision support tool to improve the quality of communication and decision-making in individuals with atrial fibrillation
- PMID: 22861171
- PMCID: PMC3419306
- DOI: 10.1111/j.1532-5415.2012.04080.x
A pilot randomized controlled trial of a decision support tool to improve the quality of communication and decision-making in individuals with atrial fibrillation
Abstract
Objectives: To design a tool for nonvalvular atrial fibrillation (NVAF) to inform individuals of their individual stroke and bleeding risks, assist in clarifying priorities, and promote communication.
Design: Clustered randomized controlled trial.
Setting: Primary care clinics.
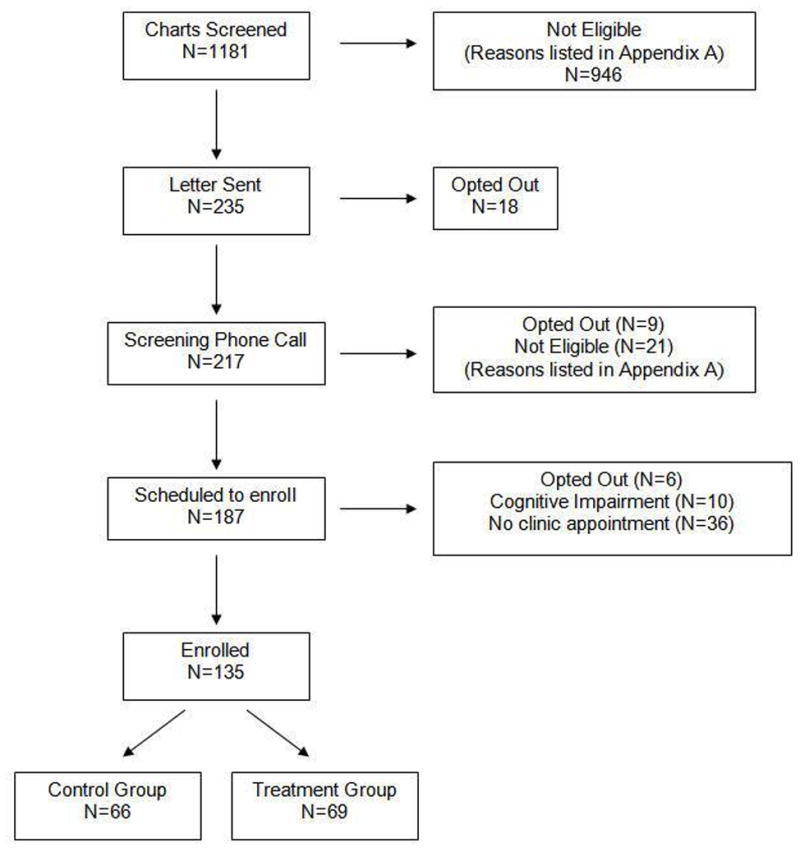
Participants: Individuals with NVAF (N = 135).
Intervention: Completion of tool before regularly scheduled visit.
Measurements: Primary outcomes included the 100-point informed and values clarity subscales of the decisional conflict scale (lower scores indicate individual is more informed and has greater clarity). Secondary outcomes included knowledge, patient-clinician communication, and change in treatment.
Results: Sixty-nine individuals were enrolled in the intervention group and 66 in the control group. After their visit, intervention participants had lower scores on the informed (mean difference = -11.9, 95% confidence interval (CI) = -21.1 to -2.7) and values clarity subscales (mean difference = -14.6, 95% CI = -22.6 to -6.6). Greater proportions of intervention participants knew medications for reducing stroke risk (61% vs 31%, P < .001) and side effects (49% vs 37%, P = .07). Stroke (71% vs 12%) and bleeding risk (69% vs 20%) were discussed more frequently in the intervention than control group (P < .001). Five intervention participants expressed a preference for medication that was not concordant with their current treatment plan. There was no change in treatment plan in either group.
Conclusion: The tool was effective in improving perceived and actual knowledge and values clarity and in increasing physician-patient communication but did not change treatment.
© 2012, Copyright the Authors Journal compilation © 2012, The American Geriatrics Society.
Figures
References
-
- O’Connor AM, Bennett CL, Stacey D, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database System Rev. 2009:CD001431. - PubMed
-
- Kaplan SH, Gandek B, Greenfield S, et al. Patient and visit characteristics related to physicians’ participatory decision-making style: Results from the Medical Outcomes Study. Med Care. 1995;33:1176–1187. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
