

Radiation and smoking effects on lung cancer incidence by histological types among atomic bomb survivors
- PMID: 22862780
- PMCID: PMC4031371
- DOI: 10.1667/rr2819.1
Radiation and smoking effects on lung cancer incidence by histological types among atomic bomb survivors
Abstract
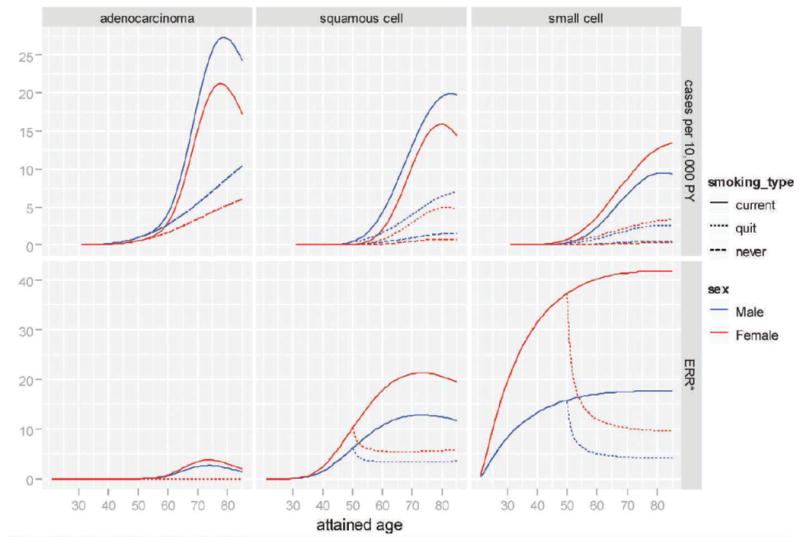
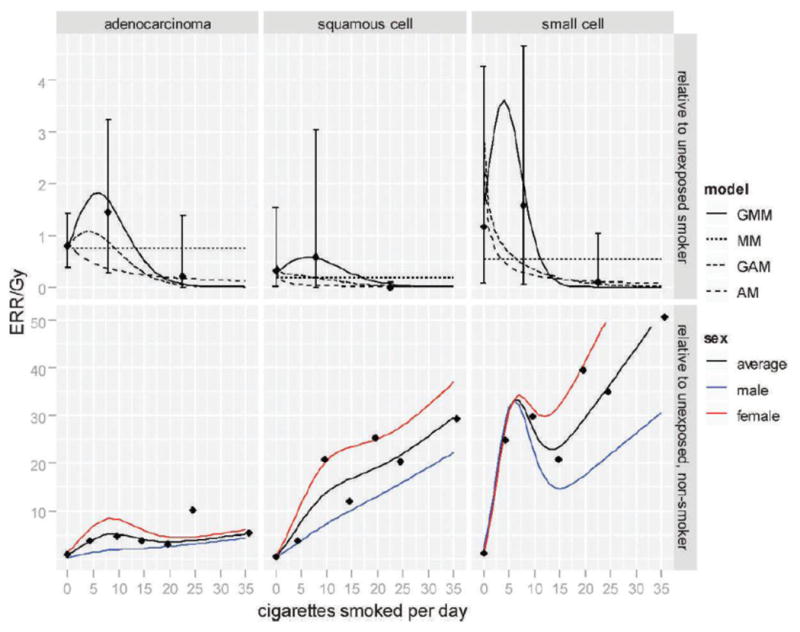
While the risk of lung cancer associated separately with smoking and radiation exposure has been widely reported, it is not clear how smoking and radiation together contribute to the risk of specific lung cancer histological types. With individual smoking histories and radiation dose estimates, we characterized the joint effects of radiation and smoking on type-specific lung cancer rates among the Life Span Study cohort of Japanese atomic bomb survivors. Among 105,404 cohort subjects followed between 1958 and 1999, 1,803 first primary lung cancer incident cases were diagnosed and classified by histological type. Poisson regression methods were used to estimate excess relative risks under several interaction models. Adenocarcinoma (636 cases), squamous-cell carcinoma (330) and small-cell carcinoma (194) made up 90% of the cases with known histology. Both smoking and radiation exposure significantly increased the risk of each major lung cancer histological type. Smoking-associated excess relative risks were significantly larger for small-cell and squamous-cell carcinomas than for adenocarcinoma. The gender-averaged excess relative risks per 1 Gy of radiation (for never-smokers at age 70 after radiation exposure at age 30) were estimated as 1.49 (95% confidence interval 0.1-4.6) for small-cell carcinoma, 0.75 (0.3-1.3) for adenocarcinoma, and 0.27 (0-1.5) for squamous-cell carcinoma. Under a model allowing radiation effects to vary with levels of smoking, the nature of the joint effect of smoking and radiation showed a similar pattern for different histological types in which the radiation-associated excess relative risk tended to be larger for moderate smokers than for heavy smokers. However, in contrast to analyses of all lung cancers as a group, such complicated interactions did not describe the data significantly better than either simple additive or multiplicative interaction models for any of the type-specific analyses.
Figures
References
-
- Thun MJ, Lally CA, Flannery JT, Calle EE, Flanders WD, Heath CW., Jr Cigarette smoking and changes in the histopathology of lung cancer. J Natl Cancer Inst. 1997;89:1580–86. - PubMed
-
- Janssen-Heijnen ML, Coebergh JW. Trends in incidence and prognosis of the histological subtypes of lung cancer in North America, Australia, New Zealand and Europe. Lung Cancer. 2001;31:123–37. - PubMed
-
- Ito H, Matsuo K, Tanaka H, Koestler DC, Ombao H, Fulton J, et al. Nonfilter and filter cigarette consumption and the incidence of lung cancer by histological type in Japan and the United States: analysis of 30-year data from population-based cancer registries. Int J Cancer. 2011;128:1918–28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
