

Hypoxia induces gefitinib resistance in non-small-cell lung cancer with both mutant and wild-type epidermal growth factor receptors
- PMID: 22863020
- PMCID: PMC7659171
- DOI: 10.1111/j.1349-7006.2012.02408.x
Hypoxia induces gefitinib resistance in non-small-cell lung cancer with both mutant and wild-type epidermal growth factor receptors
Abstract
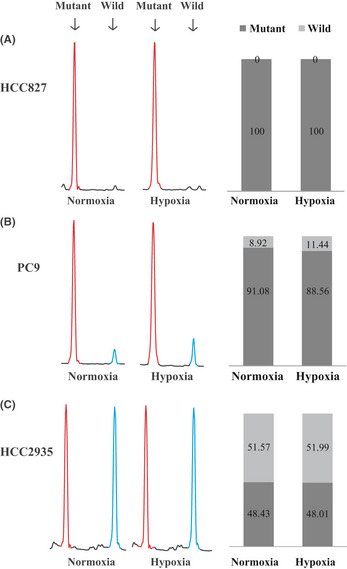
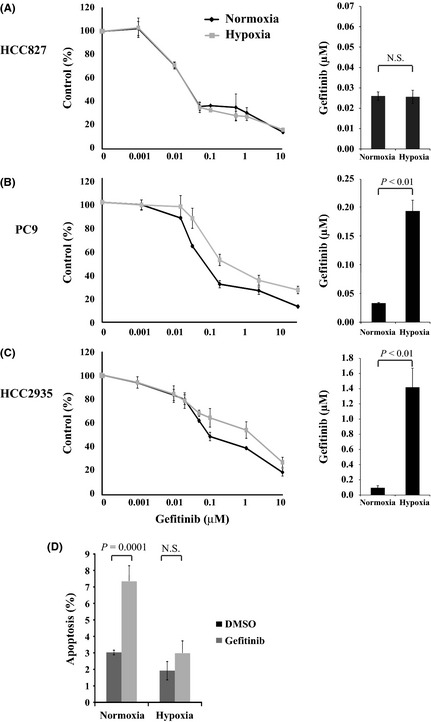
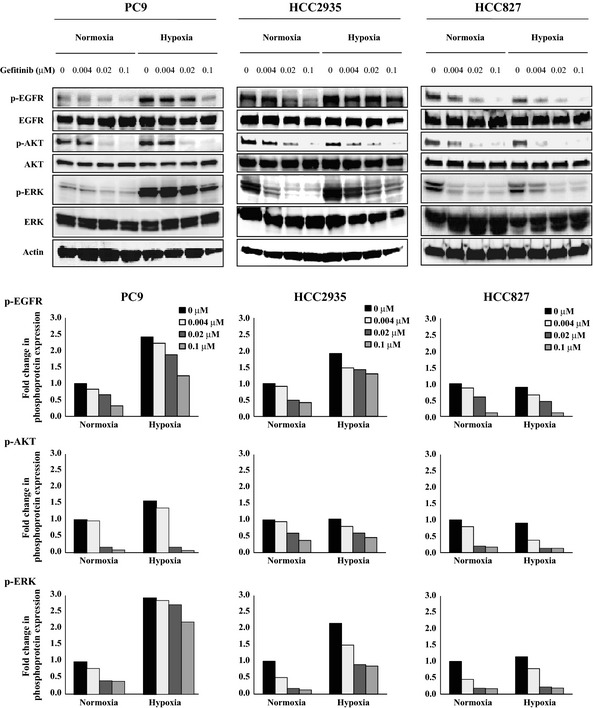
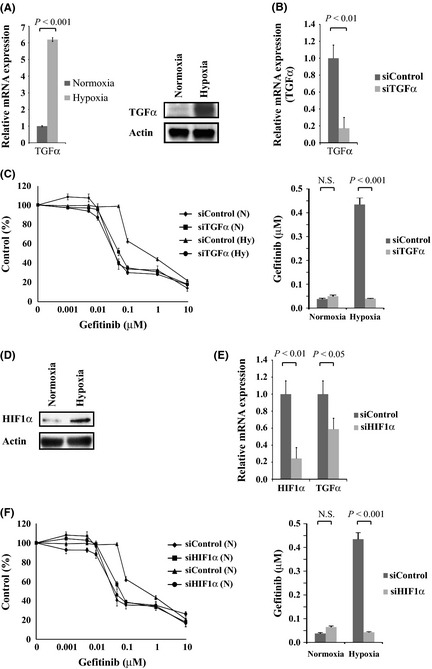
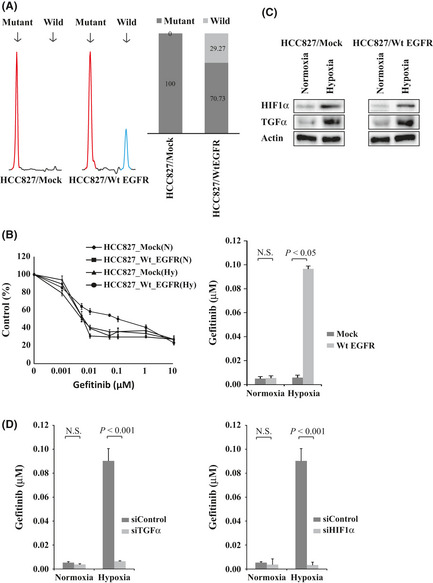
Somatic mutations in the epidermal growth factor receptor (EGFR) gene, such as exon 19 deletion mutations, are important factors in determining therapeutic responses to gefitinib in non-small-cell lung cancer (NSCLC). However, some patients have activating mutations in EGFR and show poor responses to gefitinib. In this study, we examined three NSCLC cell lines, HCC827, PC9, and HCC2935, that expressed an EGFR exon 19 deletion mutation. All cells expressed mutant EGFR, but the PC9 and HCC2935 cells also expressed wild-type EGFR. The HCC827 cells were highly sensitive to gefitinib under both normoxia and hypoxia. However, the PC9 and HCC2935 cells were more resistant to gefitinib under hypoxic conditions compared to normoxia. Phosphorylation of EGFR and ERK was suppressed with gefitinib treatment to a lesser extent under hypoxia. The expression of transforming growth factor-α (TGFα) was dramatically upregulated under hypoxia, and the knockdown of TGFα or hypoxia-inducible factor-1α (HIF1α) reversed the resistance to gefitinib in hypoxic PC9 and HCC2935 cells. Finally, introduction of the wild-type EGFR gene into the HCC827 cells caused resistance to gefitinib under hypoxia. This phenomenon was also reversed by the knockdown of TGFα or HIF1α. Our results indicate that hypoxia causes gefitinib resistance in EGFR-mutant NSCLC through the activation of wild-type EGFR mediated by the upregulation of TGFα. The presence of wild-type and mutant EGFR along with tumor hypoxia are important factors that should be considered when treating NSCLC patients with gefitinib.
© 2012 Japanese Cancer Association.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010; 60: 277–300. - PubMed
-
- Ohsaki Y, Tanno S, Fujita Y et al Epidermal growth factor receptor expression correlates with poor prognosis in non‐small cell lung cancer patients with p53 overexpression. Oncol Rep 2000; 7: 603–7. - PubMed
-
- Hirsch FR, Varella‐Garcia M, Bunn PA Jr et al Epidermal growth factor receptor in non‐small‐cell lung carcinomas: correlation between gene copy number and protein expression and impact on prognosis. J Clin Oncol 2003; 21: 3798–807. - PubMed
-
- Sharma SV, Bell DW, Settleman J, Haber DA. Epidermal growth factor receptor mutations in lung cancer. Nat Rev Cancer 2007; 7: 169–81. - PubMed
-
- Rusch V, Baselga J, Cordon‐Cardo C et al Differential expression of the epidermal growth factor receptor and its ligands in primary non‐small cell lung cancers and adjacent benign lung. Cancer Res 1993; 53: 2379–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
