

Head and neck squamous carcinomas with exophytic and endophytic type of growth have the same prognosis after surgery and adjuvant radiotherapy
- PMID: 22865105
- PMCID: PMC3818094
- DOI: 10.1007/s00405-012-2117-1
Head and neck squamous carcinomas with exophytic and endophytic type of growth have the same prognosis after surgery and adjuvant radiotherapy
Abstract
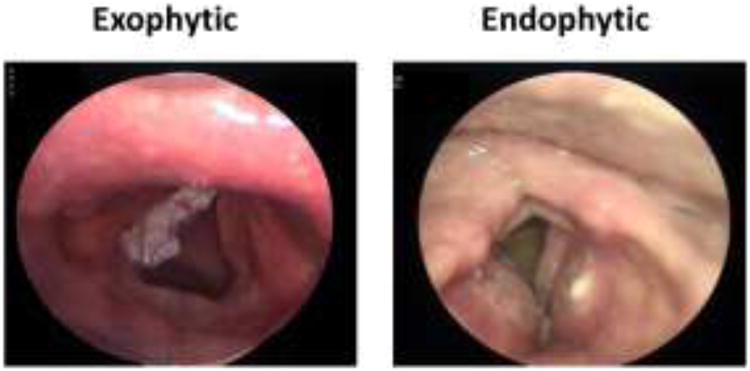
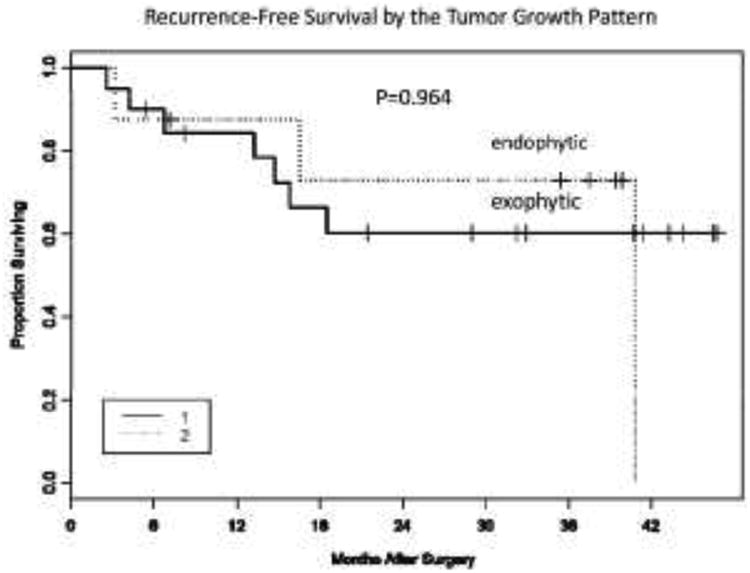
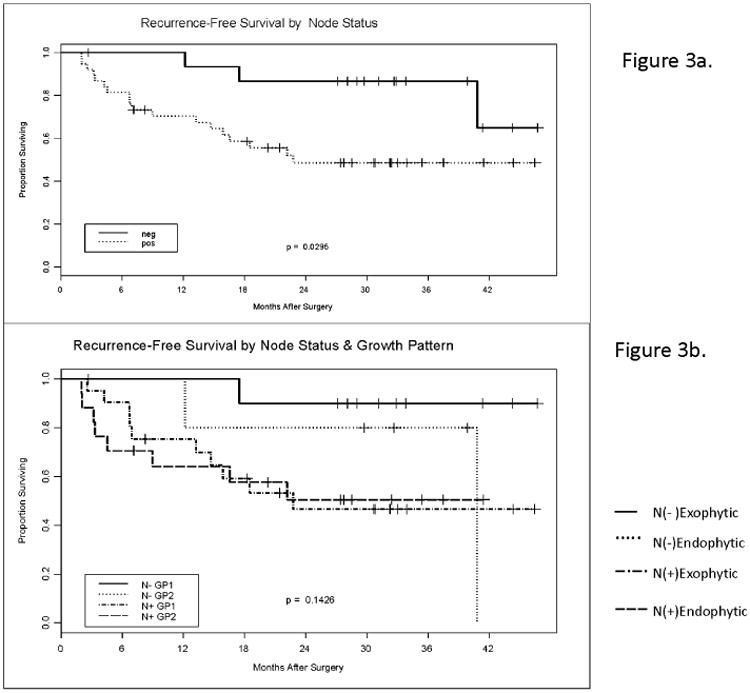
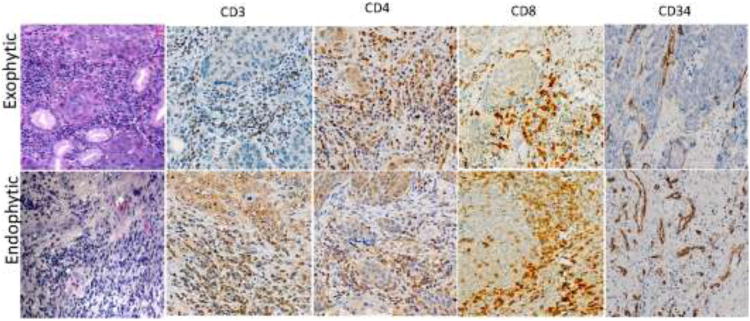
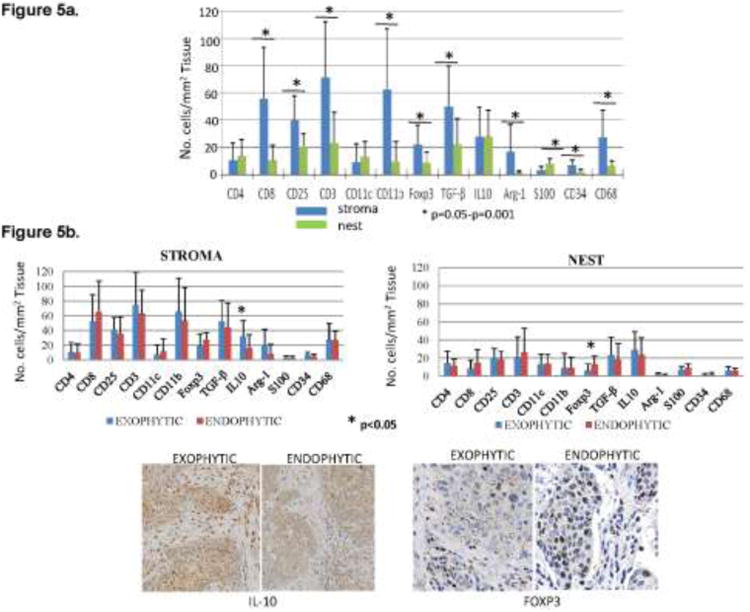
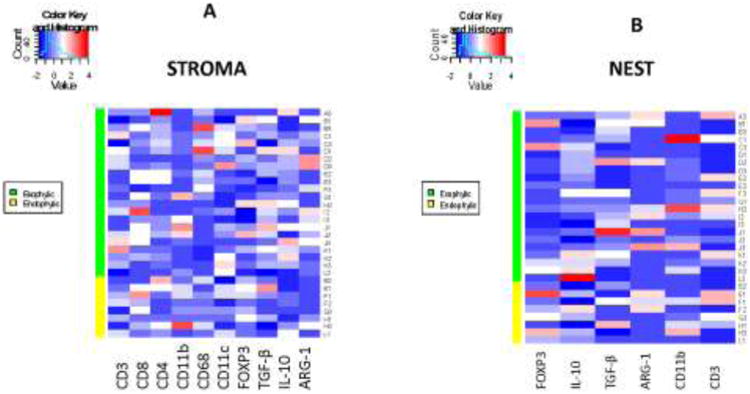
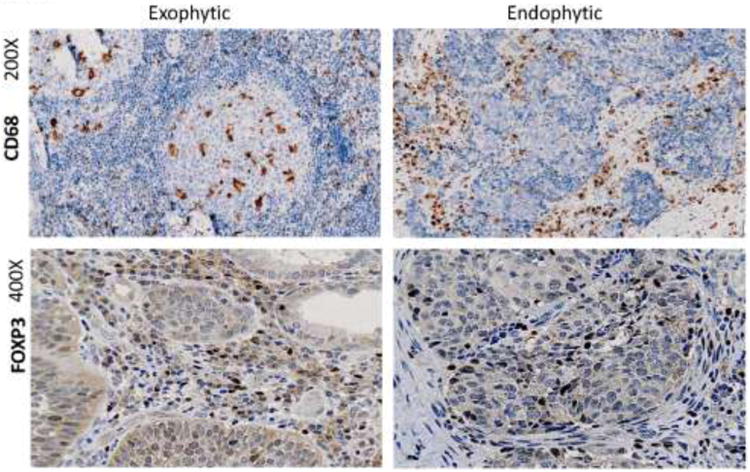
Head and neck squamous cell carcinomas (HNSCC) are characterized by exophytic or endophytic growth. We hypothesized that the growth pattern predicts outcome and associates with distinct clinical and immunological profiles. Tumors obtained from 60 HNSCC patients treated with surgery and adjuvant radiotherapy were identified as exophytic or endophytic. Recurrence-free survival (RFS) at 42 months was determined. In a subsets of 30 patients (22 exophytic and 8 endophytic) tumor stroma and parenchyma were evaluated for infiltrating CD4(+) and CD8(+) T, dendritic, myeloid and FOXP3(+) regulatory T cells (Treg) and expression of immunosuppressive cytokines by immunohistochemistry. The localization and frequency of positive cells were determined microscopically and analyzed by hierarchical clustering to distinguish exophytic versus endophytic tumors. 34/60 patients had exophytic and 26/60 endophytic tumors. No differences in clinicopathologic data, disease progression or RFS were seen between the two cohorts. Infiltrates of CD3(+)CD8(+) T cells were larger in endophytic than exophytic tumors, while FOXP3(+) Treg, TGF-β(+), IL-10(+), Arg-1(+), CD11b(+) cells were equally prominent in both. FOXP3(+) Treg accumulated in endophytic tumor nests, while the exophytic tumor stroma was enriched in IL-10(+) cells (both at p < 0.05). Hierarchical clustering based on immunophenotyping failed to identify different clusters in these two tumor types. However, CD68(+) macrophages and FOXP3(+) Treg showed a distinct distribution. The HNSCC growth pattern did not predict RFS. Although higher numbers and differences in localization of immunosuppressive cells in endophytic versus exophytic tumors were observed, no significant relationship was established between the growth pattern and the immune profile of infiltrating lymphocytes.
Conflict of interest statement
Figures
Similar articles
-
Tumor infiltrating lymphocytes and survival in patients with head and neck squamous cell carcinoma.Head Neck. 2016 Jul;38(7):1074-84. doi: 10.1002/hed.24406. Epub 2016 Feb 16. Head Neck. 2016. PMID: 26879675 Free PMC article.
-
Blockade of adenosine A2A receptor enhances CD8+ T cells response and decreases regulatory T cells in head and neck squamous cell carcinoma.Mol Cancer. 2017 Jun 7;16(1):99. doi: 10.1186/s12943-017-0665-0. Mol Cancer. 2017. PMID: 28592285 Free PMC article.
-
Dynamics of regulatory T cells (Tregs ) in patients with oral squamous cell carcinoma.J Surg Oncol. 2017 Dec;116(8):1103-1113. doi: 10.1002/jso.24782. Epub 2017 Aug 22. J Surg Oncol. 2017. PMID: 28833201
-
Digital pathology-aided assessment of tumor-infiltrating T lymphocytes in advanced stage, HPV-negative head and neck tumors.Cancer Immunol Immunother. 2020 Apr;69(4):581-591. doi: 10.1007/s00262-020-02481-3. Epub 2020 Jan 24. Cancer Immunol Immunother. 2020. PMID: 31980916 Free PMC article.
-
Immune suppression in head and neck cancers: a review.Clin Dev Immunol. 2010;2010:701657. doi: 10.1155/2010/701657. Epub 2011 Mar 10. Clin Dev Immunol. 2010. PMID: 21437225 Free PMC article. Review.
Cited by
-
EGFR signaling controls directionality of epithelial multilayer formation upon loss of cell polarity.EMBO J. 2023 Dec 11;42(24):e113856. doi: 10.15252/embj.2023113856. Epub 2023 Nov 13. EMBO J. 2023. PMID: 37953688 Free PMC article.
-
Machine Learning Analysis of Gaze Data for Enhanced Precision in Diagnosing Oral Mucosal Diseases.J Clin Med. 2023 Dec 26;13(1):136. doi: 10.3390/jcm13010136. J Clin Med. 2023. PMID: 38202143 Free PMC article.
-
Case Report: Hidden Oral Squamous Cell Carcinoma in Oral Somatic Symptom Disorder.Front Psychiatry. 2021 Apr 1;12:651871. doi: 10.3389/fpsyt.2021.651871. eCollection 2021. Front Psychiatry. 2021. PMID: 33868058 Free PMC article.
-
Prognostic impact of immune microenvironment in laryngeal and pharyngeal squamous cell carcinoma: Immune cell subtypes, immuno-suppressive pathways and clinicopathologic characteristics.Oncotarget. 2017 Mar 21;8(12):19310-19322. doi: 10.18632/oncotarget.14242. Oncotarget. 2017. PMID: 28038471 Free PMC article.
-
Quantitative magnetic resonance imaging responses in head and neck cancer patients treated with magnetic resonance-guided hypofractionated radiation therapy.Phys Imaging Radiat Oncol. 2025 Jan 2;33:100693. doi: 10.1016/j.phro.2024.100693. eCollection 2025 Jan. Phys Imaging Radiat Oncol. 2025. PMID: 39877149 Free PMC article.
References
-
- Forastiere A, Koch W, Trotti A, Sidransky D. Head and neck cancer. N Engl J Med. 2001;345:1890–1900. - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Brockstein BE. Management of recurrent head and neck cancer: recent progress and future directions. Drugs. 2011;71:1551–1559. - PubMed
-
- Chin D, Boyle GM, Porceddu S, Theile DR, Parsons PG, Coman WB. Head and neck cancer: past, present and future. Exp Rev Anticancer Ther. 2006;6:1111–1118. - PubMed
-
- Jakobsson PA, Eneroth CM, Killander D, Moberger G, Martensson B. Histologic classification and grading of malignancy in carcinoma of the larynx. Acta Radiol Ther Phys Biol. 1973;12:1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
