

Independent and interactive effects of preload and afterload on the pump function of the isolated lymphangion
- PMID: 22865389
- PMCID: PMC3469707
- DOI: 10.1152/ajpheart.01098.2011
Independent and interactive effects of preload and afterload on the pump function of the isolated lymphangion
Abstract
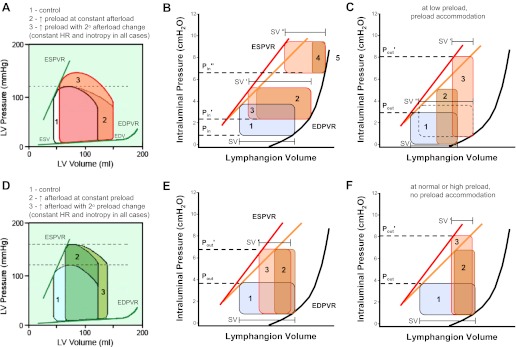
We tested the responses of single, isolated lymphangions to selective changes in preload and the effects of changing preload on the response to an imposed afterload. The methods used were similar to those described in our companion paper. Step-wise increases in input pressure (P(in); preload) over a pressure range between 0.5 and 3 cmH(2)O, at constant output pressure (P(out)), led to increases in end-diastolic diameter, decreases in end-systolic diameter, and increases in stroke volume. From a baseline of 1 cmH(2)O, P(in) elevation by 2-7 cmH(2)O consistently produced an immediate fall in stroke volume that subsequently recovered over a time course of 2-3 min. Surprisingly, this adaptation was associated with an increase in the slope of the end-systolic pressure-volume relationship, indicative of an increase in contractility. Lymphangions subjected to P(out) levels exceeding their initial ejection limit would often accommodate by increasing diastolic filling to strengthen contraction sufficiently to match P(out). The lymphangion adaptation to various pressure combinations (P(in) ramps with low or high levels of P(out), P(out) ramps at low or intermediate levels of P(in), and combined P(in) + P(out) ramps) were analyzed using pressure-volume data to calculate stroke work. Under relatively low imposed loads, stroke work was maximal at low preloads (P(in) ∼2 cmH(2)O), whereas at more elevated afterloads, the optimal preload for maximal work displayed a broad plateau over a P(in) range of 5-11 cmH(2)O. These results provide new insights into the normal operation of the lymphatic pump, its comparison with the cardiac pump, and its potential capacity to adapt to increased loads during edemagenic and/or gravitational stress.
Figures







References
-
- Aukland K. Why don't our feet swell in the upright position? News Physiol Sci 9: 214–219, 1994
-
- Benoit JN, Zawieja DC, Goodman AH, Granger HJ. Characterization of intact mesenteric lymphatic pump and its responsiveness to acute edemagenic stress. Am J Physiol Heart Circ Physiol 257: H2059–H2069, 1989 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical