

Case Reports
doi: 10.4103/0976-3147.98246.
Cerebellopontine angle ependymoma in a 2-year- old child
Affiliations
- PMID: 22865982
- PMCID: PMC3410001
- DOI: 10.4103/0976-3147.98246
Item in Clipboard
Case Reports
Cerebellopontine angle ependymoma in a 2-year- old child
J Neurosci Rural Pract.
2012 May.
Abstract
The management of cerebellopontine angle (CPA) ependymoma in children below 3 years of age is challenging. In addition to the rare occurrence of disease, the difficulty also lies in achieving gross total resection and providing radiotherapy in this subset of patients. We describe a case of CPA ependymoma in a 2-year-old child. Gross total excision was achieved followed by administration of radiotherapy. In this article, a review of literature for this rare entity and the difficulties faced in the surgery and adjuvant treatment has been discussed.
Keywords: Cerebellopontine angle; children; ependymoma.
Conflict of interest statement
Figures
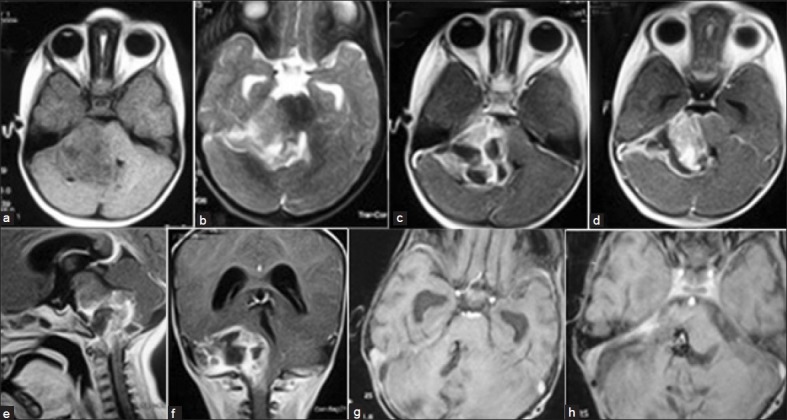
(a) Axial T1-weighted image showing iso-hypointense lesion in the right cerebellopontine (CP) angle. (b) Axial T2-weighted image showing the extra-axial hyperintense lesion in the CP angle. (c and d) Contrast axial image showing the enhancing lesion with cystic areas compressing the brain stem and fourth ventricle. (e) Sagittal contrast magnetic resonance imaging (MRI) section showing the extent of lesion. (f) Coronal contrast MRI section showing the extent of lesion. (g) Axial contrast MRI showing gross total excision and opened fourth ventricle. (h) Axial contrast MRI showing gross total excision and the foramen of Luschka is clear
Similar articles
-
Adult cerebellopontine angle ependymoma presenting as an isolated cisternal mass: A case report.J Med Imaging Radiat Sci. 2020 Dec;51(4):689-693. doi: 10.1016/j.jmir.2020.08.007. Epub 2020 Sep 2. J Med Imaging Radiat Sci. 2020. PMID: 32888857
-
Cerebellopontine angle ependymoma presenting as isolated hearing loss in an elderly patient: A case report and literature review.Surg Neurol Int. 2021 Nov 23;12:572. doi: 10.25259/SNI_781_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34877058 Free PMC article.
-
Microsurgical Resection of Anaplastic Ependymoma of the Cerebellopontine Angle in an Adult: 3-Dimensional Operative Video.Oper Neurosurg. 2019 Mar 1;16(3):E91. doi: 10.1093/ons/opy217. Oper Neurosurg. 2019. PMID: 30295880
-
Surgical management of primary and secondary pilocytic astrocytoma of the cerebellopontine angle (in adults and children) and review of the literature.Neurosurg Rev. 2021 Apr;44(2):1083-1091. doi: 10.1007/s10143-020-01293-4. Epub 2020 Apr 15. Neurosurg Rev. 2021. PMID: 32297071 Free PMC article. Review.
-
Low-grade ependymoma with late metastasis: autopsy case study and literature review.Childs Nerv Syst. 2015 Sep;31(9):1565-72. doi: 10.1007/s00381-015-2744-0. Epub 2015 May 10. Childs Nerv Syst. 2015. PMID: 25957762 Review.
Cited by
-
Posterior Fossa Ependymoma in a Child with Extensive Chondro-Osseous Metaplasia Occurring at Cerebellopontine Angle and Masquerading as a Vestibular Schwannoma: An Exceptionally Rare Clinicopathological Manifestation with Review of Literature.J Neurol Surg Rep. 2024 Aug 29;85(3):e132-e137. doi: 10.1055/a-2372-6701. eCollection 2024 Jul. J Neurol Surg Rep. 2024. PMID: 39211009 Free PMC article.
References
-
- Sanford SA, Merchant TE, Lee MZ, Kun LE, Boop FA. Advances in surgical techniques for resection of childhood cerebello-pontine angle ependymomas are key to survival. Childs Nerv Syst. 2009;25:1229–40. - PubMed
-
- Holst B, Grunwald IQ, Brill G, Reith W. Differential diagnosis of space demands in the cerebellopontine angle. Radiologe. 2004;44:1113–36. - PubMed
-
- Shapey J, Barazi S, Bodi I, Thomas N. Myxopapillary ependymoma of the cerebellopontine angle: Retrograde metastasis or primary tumour? Br J Neurosurg. 2011;25:122–3. - PubMed
-
- Sparaco M, Morelli L, Piscioli I, Donato S, Catalucci A, Licci S. Primary myxopapillary ependymoma of the cerebellopontine angle: Report of a case. Neurosurg Rev. 2009;32:241–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources