

Congenital cystic lesions of the lung: congenital cystic adenomatoid malformation and bronchopulmonary sequestration
Affiliations
- PMID: 22866187
- PMCID: PMC3410507
Item in Clipboard
Congenital cystic lesions of the lung: congenital cystic adenomatoid malformation and bronchopulmonary sequestration
Rev Obstet Gynecol.
2012.
Abstract
Congenital cystic lesions of the lung in fetuses are rare. The most common malformations of the lower respiratory tract are congenital cystic adenomatoid malformation and bronchopulmonary sequestration. With the increased use of obstetric ultrasound, cystic lung lesions are detected more often antenatally, which allows for proper planning of peripartum and neonatal management. This article discusses a range of diagnostic and management options.
Keywords: Bronchopulmonary sequestration; Congenital cystic adenomatoid malformation; Congenital pulmonary airway malformation; Pulmonary hypoplasia.
Figures
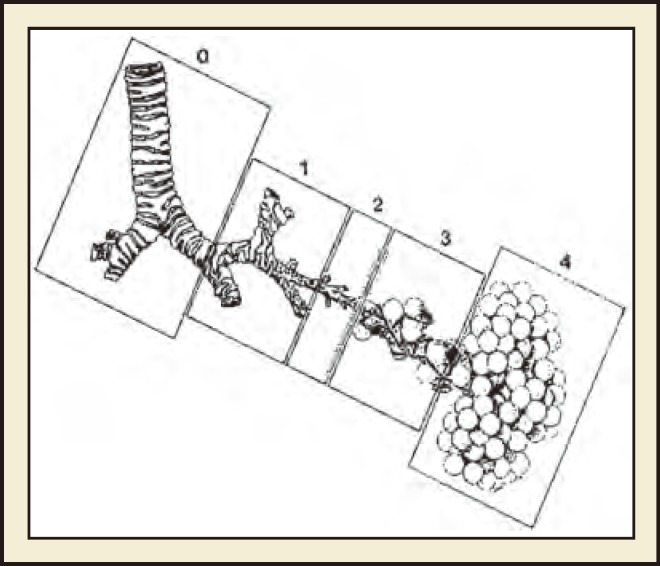
Congenital cystic adenomatoid malformation classification based on presumed site of development of the malformation. 0 = tracheobronchial, 1 = bronchial/bronchiolar, 2 = bronchiolar, 3 = bronchiolar/alveolar, 4 5 distal acinar. Stocker JT, Fetal Pediatr Pathol. 2009;28:155–184, copyright © 2009, Informa Healthcare. Reproduced with permission from Informa Healthcare.
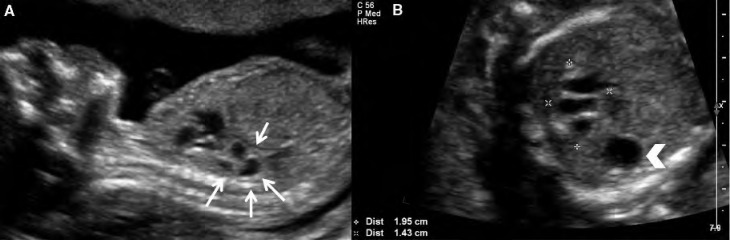
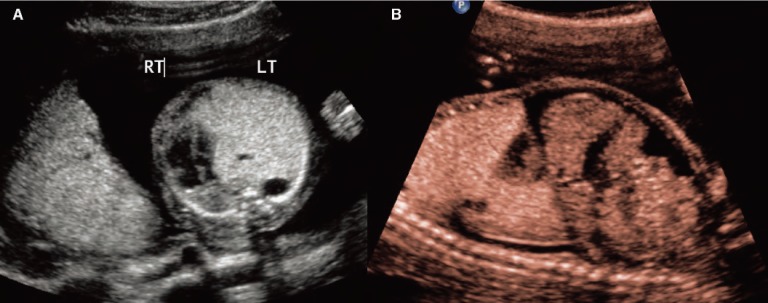
Case 1. Type 2 congenital cystic adenomatoid malformation (CCAM). A, Sagittal image of a fetus at 24 weeks with Type 2 CCAM located in the posterior chest (arrows). B, Transverse image with measurements showing the inferior extent of the lesion. The mass is multicystic and located inferior and posterior to the heart. Arrowhead indicates the stomach.
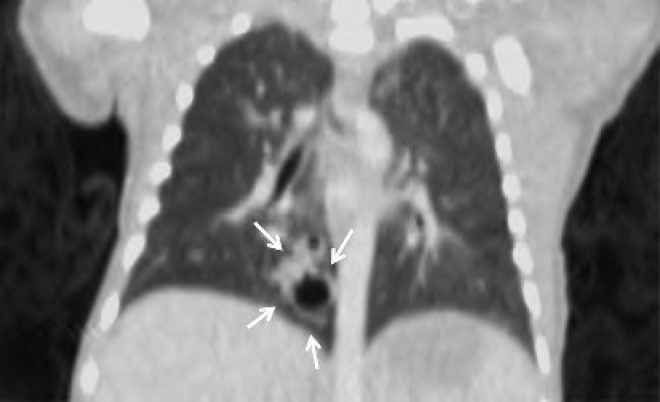
Computed tomography scan of the neonate in Case 1, performed on day of life 1. There is a 0.9 × 0.9 cm mass with several cysts within the medial segment of the right lower lobe. No systemic vessels can be seen supplying the mass. Findings are consistent with a Type 2 congenital cystic adenomatoid malformation.
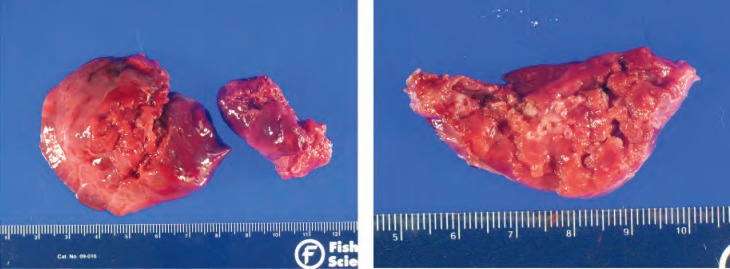
Gross image of the Type 2 congenital cystic adenomatoid malformation seen in Figure 1. The ascites resolved by 24 weeks and the fetus was stable until delivery. The neonate underwent right lower lobe lobectomy on day of life 2 due to persistent mediastinal shift.
Case 2. A, Transverse image of a fetus at 22 weeks with Type 2 congenital cystic adenomatoid malformation (CCAM). The heart has been displaced into the right thorax due to the large CCAM. Note the two cysts within the echogenic mass of the CCAM. B, Sagittal image of the fetus demonstrating ascites. Note the liver with surrounding fluid. The ascites resolved 3 weeks later and the mass was resected on day of life 2 due to persistent mediastinal shift.

Computed tomography scan of the neonate in Case 2 on day of life 1. Findings are compatible with cystic adenomatoid malformation of the left upper lobe with associated marked hyperinflation causing rightward mediastinal shift and deviation of the descending thoracic aorta. Note less marked involvement of the basilar segments of the left lower lobe. The patient underwent left upper lobe lobectomy at 4 months of life (see Figure 7).
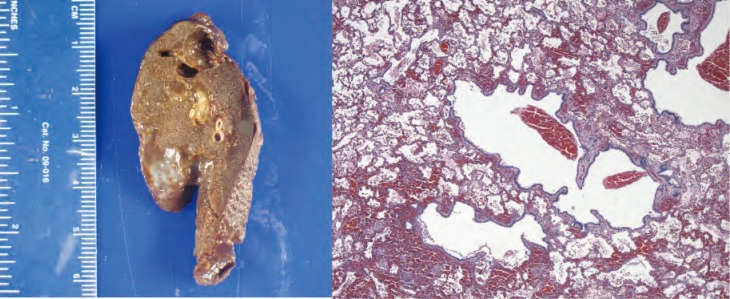
Gross and histologic specimens of the patient in Case 2; the patient underwent left upper lobe lobectomy at 4 months of life. Histology shows several small evenly spaced cystic structures of relatively uniform size are present in the area illustrated. The cysts are lined by ciliated cuboidal to columnar epithelium that overlies a fine fibromuscular layer, barely visible at this magnification. Image courtesy of A. Brian West, MD, FRCPath, Yale School of Medicine, New Haven, CT.

Case 3. Sagittal image of a fetus at 20 weeks with Type 3 congenital cystic adenomatoid malformation demonstrating its position posterior and to the left of the heart. The heart is displaced to the right.

Case 3. Severe Type 3 congenital cystic adenomatoid malformation. The lesion has become large enough to compress the cardiac anatomy. This fetus is at risk for hydrops.

Case 4. Axial image of a fetus with bronchopulmonary sequestration demonstrating the fourchamber view and the proximity to the descending aorta. The fetus never developed hydrops and the mass was resected electively at age 3 months.
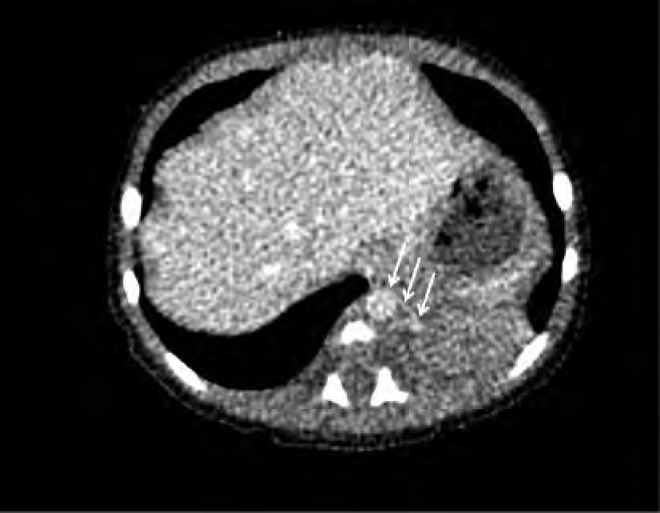
Computed tomography scan of the neonate in Case 4 on day of life 2. There is a solid soft tissue density within the left lower lobe measuring approximately 3 cm 3 2 cm. A small vessel arising from the descending aorta is seen supplying this solid mass (arrows); findings are consistent with sequestration. The baby underwent resection of the mass at 3 months of age.
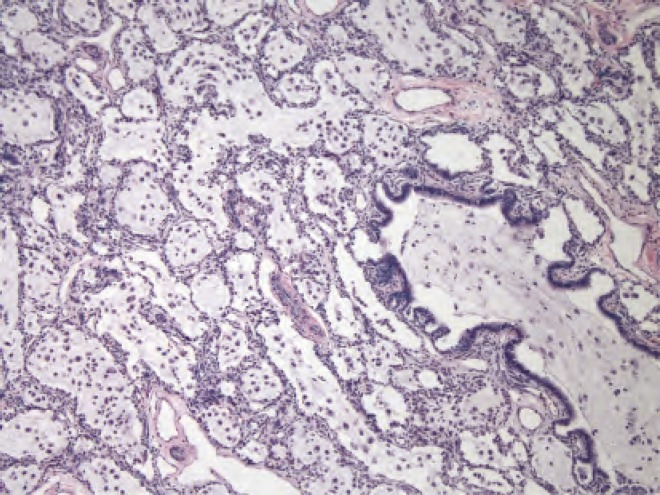
Histology slide from the resection in Case 4. Dilated airways in this part of the specimen are filled with pale-staining mucin secondary to obstruction. Image courtesy of A. Brian West, MD, FRCPath, Yale School of Medicine, New Haven, CT.
References
-
- Laberge JM, Flageole H, Pugash D, et al. Outcome of the prenatally diagnosed congenital cystic adenomatoid lung malformation: a Canadian experience. Fetal Diagn Ther. 2001;16:178–186. - PubMed
-
- Gornall AS, Budd JL, Draper ES, et al. Congenital cystic adenomatoid malformation: accuracy of prenatal diagnosis, prevalence and outcome in a general population. Prenat Diagn. 2003;23:997–1002. - PubMed
-
- Bianchi DW, Crombleholme TM, D’Alton ME, Malone FE, editors. Fetology. Diagnosis and Management of the Fetal Patient. 2nd ed. New York, NY: McGraw Hill; 2010.
-
- Cass DL, Crombleholme TM, Howell LJ, et al. Cystic lung lesions with systemic arterial blood supply: a hybrid of congenital cystic adenomatoid malformation and bronchopulmonary sequestration. J Pediatr Surg. 1997;32:986–990. - PubMed
-
- Davenport M, Warne SA, Cacciaguerra S, et al. Current outcome of antenally diagnosed cystic lung disease. J Pediatr Surg. 2004;39:549–556. - PubMed
LinkOut - more resources
Full Text Sources
Medical