

Development and validation of a clinical prediction rule for chest wall syndrome in primary care
- PMID: 22866824
- PMCID: PMC3444903
- DOI: 10.1186/1471-2296-13-74
Development and validation of a clinical prediction rule for chest wall syndrome in primary care
Abstract
Background: Chest wall syndrome (CWS), the main cause of chest pain in primary care practice, is most often an exclusion diagnosis. We developed and evaluated a clinical prediction rule for CWS.
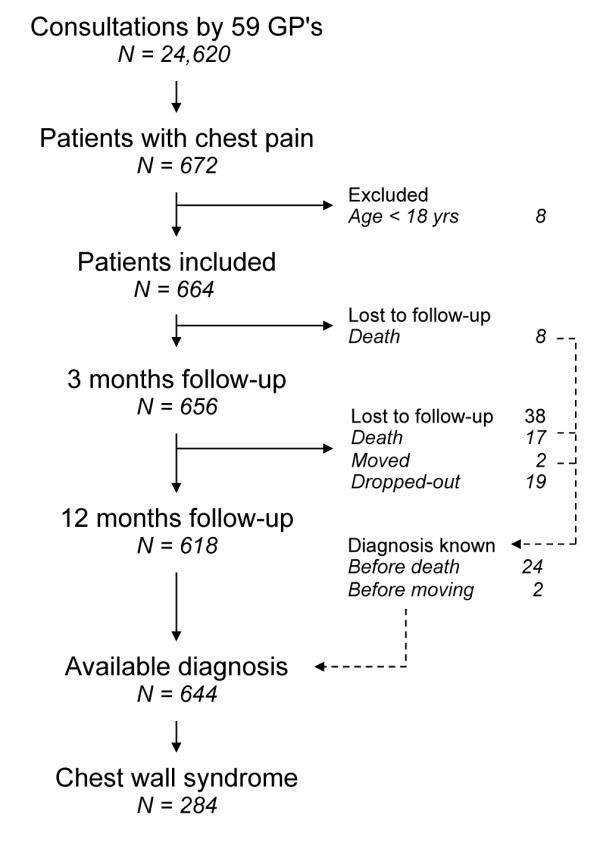
Methods: Data from a multicenter clinical cohort of consecutive primary care patients with chest pain were used (59 general practitioners, 672 patients). A final diagnosis was determined after 12 months of follow-up. We used the literature and bivariate analyses to identify candidate predictors, and multivariate logistic regression was used to develop a clinical prediction rule for CWS. We used data from a German cohort (n = 1212) for external validation.
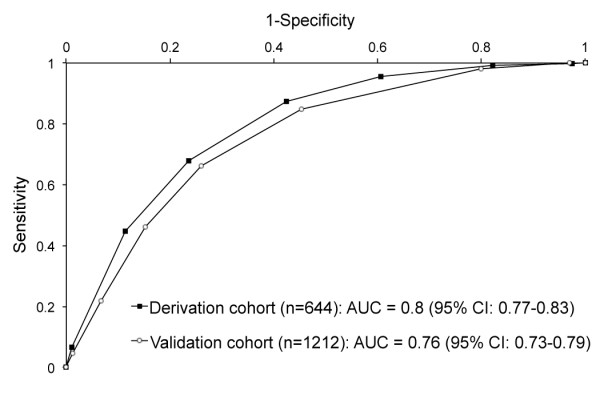
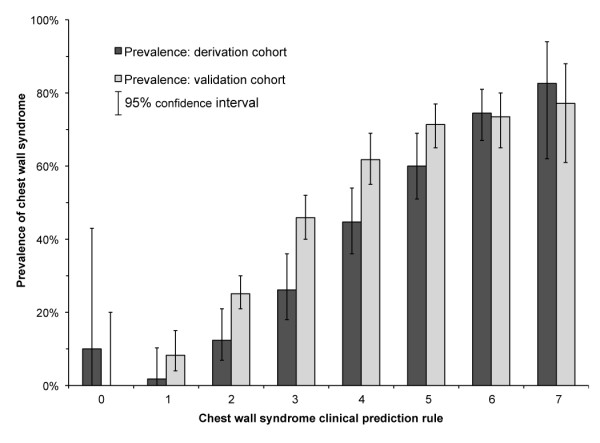
Results: From bivariate analyses, we identified six variables characterizing CWS: thoracic pain (neither retrosternal nor oppressive), stabbing, well localized pain, no history of coronary heart disease, absence of general practitioner's concern, and pain reproducible by palpation. This last variable accounted for 2 points in the clinical prediction rule, the others for 1 point each; the total score ranged from 0 to 7 points. The area under the receiver operating characteristic (ROC) curve was 0.80 (95% confidence interval 0.76-0.83) in the derivation cohort (specificity: 89%; sensitivity: 45%; cut-off set at 6 points). Among all patients presenting CWS (n = 284), 71% (n = 201) had a pain reproducible by palpation and 45% (n = 127) were correctly diagnosed. For a subset (n = 43) of these correctly classified CWS patients, 65 additional investigations (30 electrocardiograms, 16 thoracic radiographies, 10 laboratory tests, eight specialist referrals, one thoracic computed tomography) had been performed to achieve diagnosis. False positives (n = 41) included three patients with stable angina (1.8% of all positives). External validation revealed the ROC curve to be 0.76 (95% confidence interval 0.73-0.79) with a sensitivity of 22% and a specificity of 93%.
Conclusions: This CWS score offers a useful complement to the usual CWS exclusion diagnosing process. Indeed, for the 127 patients presenting CWS and correctly classified by our clinical prediction rule, 65 additional tests and exams could have been avoided. However, the reproduction of chest pain by palpation, the most important characteristic to diagnose CWS, is not pathognomonic.
Figures
Similar articles
-
Ruling out coronary artery disease in primary care: development and validation of a simple prediction rule.CMAJ. 2010 Sep 7;182(12):1295-300. doi: 10.1503/cmaj.100212. Epub 2010 Jul 5. CMAJ. 2010. PMID: 20603345 Free PMC article.
-
Ruling out coronary heart disease in primary care patients with chest pain: a clinical prediction score.BMC Med. 2010 Jan 21;8:9. doi: 10.1186/1741-7015-8-9. BMC Med. 2010. PMID: 20092615 Free PMC article.
-
Chest wall syndrome among primary care patients: a cohort study.BMC Fam Pract. 2007 Sep 12;8:51. doi: 10.1186/1471-2296-8-51. BMC Fam Pract. 2007. PMID: 17850647 Free PMC article.
-
Chest pain in general practice: a systematic review of prediction rules.BMJ Open. 2019 Feb 27;9(2):e027081. doi: 10.1136/bmjopen-2018-027081. BMJ Open. 2019. PMID: 30819715 Free PMC article.
-
Diagnosing the cause of chest pain.Am Fam Physician. 2005 Nov 15;72(10):2012-21. Am Fam Physician. 2005. PMID: 16342831 Review.
Cited by
-
Evaluating possible acute coronary syndrome in primary care: the value of signs, symptoms, and plasma heart-type fatty acid-binding protein (H-FABP). A diagnostic study.BJGP Open. 2019 Oct 29;3(3):bjgpopen19X101652. doi: 10.3399/bjgpopen19X101652. Print 2019 Oct. BJGP Open. 2019. PMID: 31581111 Free PMC article.
-
Primary care at Swiss universities--current state and perspective.BMC Res Notes. 2014 May 22;7:308. doi: 10.1186/1756-0500-7-308. BMC Res Notes. 2014. PMID: 24885148 Free PMC article.
References
-
- Yelland M, Cayley WE, Vach W. An algorithm for the diagnosis and management of chest pain in primary care. Med Clin North Am. 2010;94(2):349–374. - PubMed
-
- Epstein SE, Gerber LH, Borer JS. Chest wall syndrome. A common cause of unexplained cardiac pain. JAMA. 1979;241(26):2793–2797. - PubMed
-
- Klinkman MS, Stevens D, Gorenflo DW. Episodes of care for chest pain: a preliminary report from MIRNET. Michigan Research Network. J Fam Pract. 1994;38(4):345–352. - PubMed
-
- Buntinx F, Knockaert D, Bruyninckx R, de Blaey N, Aerts M, Knottnerus JA, Delooz H. Chest pain in general practice or in the hospital emergency department: is it the same? Fam Pract. 2001;18(6):586–589. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
