

Developing strategies for HIV-1 eradication
- PMID: 22867874
- PMCID: PMC3963166
- DOI: 10.1016/j.it.2012.07.001
Developing strategies for HIV-1 eradication
Abstract
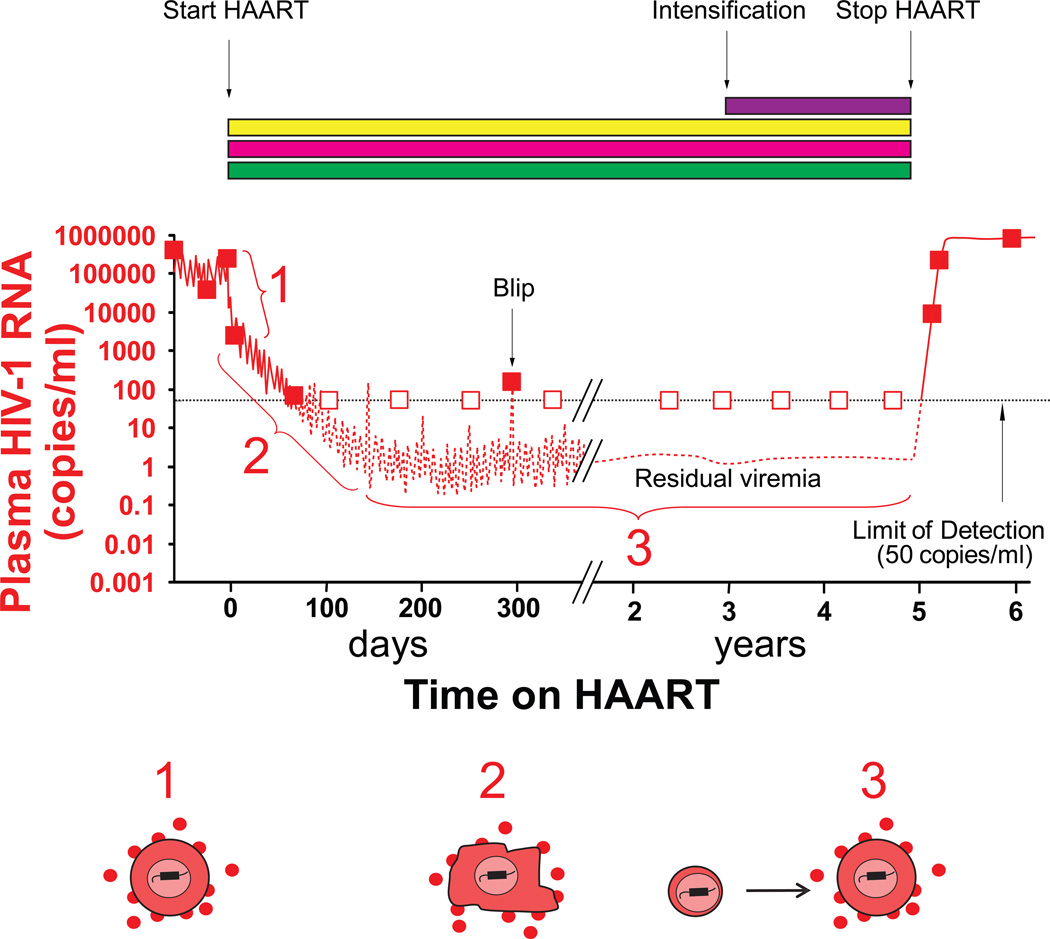
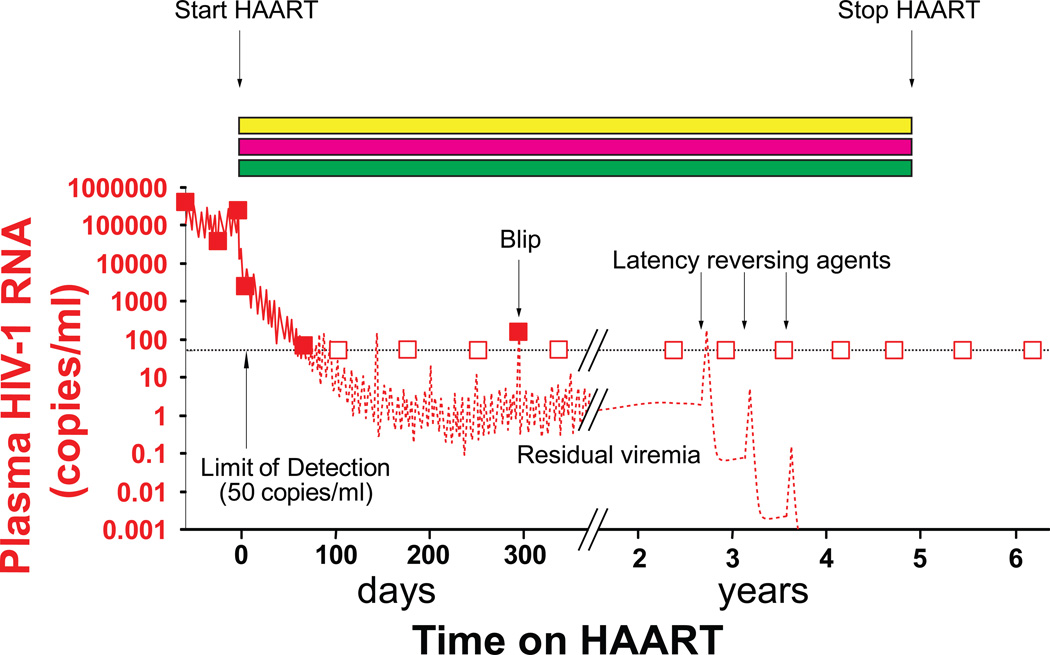
Highly active antiretroviral therapy (HAART) suppresses HIV-1 replication, transforming the outlook for infected patients. However, reservoirs of replication-competent forms of the virus persist during HAART, and when treatment is stopped, high rates of HIV-1 replication return. Recent insights into HIV-1 latency, as well as a report that HIV-1 infection was eradicated in one individual, have renewed interest in finding a cure for HIV-1 infection. Strategies for HIV-1 eradication include gene therapy and hematopoietic stem cell transplantation, stimulating host immunity to control HIV-1 replication, and targeting latent HIV-1 in resting memory CD4(+) T cells. Future efforts should aim to provide better understanding of how to reconstitute the CD4(+) T cell compartment with genetically engineered cells, exert immune control over HIV-1 replication, and identify and eliminate all viral reservoirs.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures

Similar articles
-
Reservoirs for HIV-1: mechanisms for viral persistence in the presence of antiviral immune responses and antiretroviral therapy.Annu Rev Immunol. 2000;18:665-708. doi: 10.1146/annurev.immunol.18.1.665. Annu Rev Immunol. 2000. PMID: 10837072 Review.
-
A stable latent reservoir for HIV-1 in resting CD4(+) T lymphocytes in infected children.J Clin Invest. 2000 Apr;105(7):995-1003. doi: 10.1172/JCI9006. J Clin Invest. 2000. PMID: 10749578 Free PMC article.
-
Maraviroc Is Associated with Latent HIV-1 Reactivation through NF-κB Activation in Resting CD4+ T Cells from HIV-Infected Individuals on Suppressive Antiretroviral Therapy.J Virol. 2018 Apr 13;92(9):e01931-17. doi: 10.1128/JVI.01931-17. Print 2018 May 1. J Virol. 2018. PMID: 29444937 Free PMC article.
-
Suppression of HIV replication in the resting CD4+ T cell reservoir by autologous CD8+ T cells: implications for the development of therapeutic strategies.Proc Natl Acad Sci U S A. 2001 Jan 2;98(1):253-8. doi: 10.1073/pnas.98.1.253. Proc Natl Acad Sci U S A. 2001. PMID: 11136258 Free PMC article.
-
Challenges and strategies for the eradication of the HIV reservoir.Curr Opin Immunol. 2016 Oct;42:65-70. doi: 10.1016/j.coi.2016.05.015. Epub 2016 Jun 9. Curr Opin Immunol. 2016. PMID: 27288651 Free PMC article. Review.
Cited by
-
Quantitative evaluation and optimization of co-drugging to improve anti-HIV latency therapy.Cell Mol Bioeng. 2014 Sep 1;7(3):320-333. doi: 10.1007/s12195-014-0336-9. Cell Mol Bioeng. 2014. PMID: 26191086 Free PMC article.
-
A passive-flow microfluidic device for imaging latent HIV activation dynamics in single T cells.Integr Biol (Camb). 2015 Sep;7(9):998-1010. doi: 10.1039/c5ib00094g. Epub 2015 Jul 3. Integr Biol (Camb). 2015. PMID: 26138068 Free PMC article.
-
Ephedrine enhances HIV-1 reactivation from latency through elevating tumor necrosis factor receptor II (TNFRII) expression.Heliyon. 2019 Sep 26;5(9):e02490. doi: 10.1016/j.heliyon.2019.e02490. eCollection 2019 Sep. Heliyon. 2019. PMID: 31687583 Free PMC article.
-
HIV-1 Eradication: Early Trials (and Tribulations).Trends Mol Med. 2016 Jan;22(1):10-27. doi: 10.1016/j.molmed.2015.11.004. Epub 2015 Dec 12. Trends Mol Med. 2016. PMID: 26691297 Free PMC article. Review.
-
Emerging Nanomedicine Approaches to Targeting HIV-1 and Antiretroviral Therapy.Future Virol. 2016 Feb;11(2):101-104. doi: 10.2217/fvl.15.114. Epub 2016 Feb 3. Future Virol. 2016. PMID: 28123446 Free PMC article. No abstract available.
References
-
- Chun TW, et al. In vivo fate of HIV-1-infected T cells: quantitative analysis of the transition to stable latency. Nat. Med. 1995;1:1284–1290. - PubMed
-
- Chun TW, et al. Quantification of latent tissue reservoirs and total body viral load in HIV-1 infection. Nature. 1997;387:183–188. - PubMed
-
- Finzi D, et al. Identification of a reservoir for HIV-1 in patients on highly active antiretroviral therapy. Science. 1997;278:1295–1300. - PubMed
-
- Wong JK, et al. Recovery of replication-competent HIV despite prolonged suppression of plasma viremia. Science. 1997;278:1291–1295. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
