

Thoracoscopic lobectomy has increasing benefit in patients with poor pulmonary function: a Society of Thoracic Surgeons Database analysis
- PMID: 22868367
- PMCID: PMC4089858
- DOI: 10.1097/SLA.0b013e318265819c
Thoracoscopic lobectomy has increasing benefit in patients with poor pulmonary function: a Society of Thoracic Surgeons Database analysis
Abstract
Objective: Using a national database, we asked whether video-assisted thoracoscopic surgery (VATS) lobectomy is beneficial in high-risk pulmonary patients.
Background: Single-institution series demonstrated benefit of VATS lobectomy over lobectomy via thoracotomy in poor pulmonary function patients [FEV1 (forced expiratory volume in 1 second) or DLCO (diffusion capacity of the lung to carbon monoxide) <60% predicted].
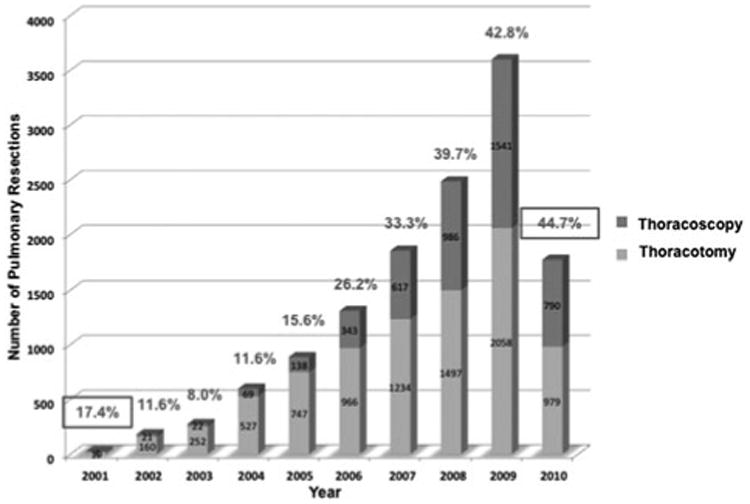
Methods: The STS General Thoracic Database was queried for patients having undergone lobectomy by either thoracotomy or VATS between 2000 and 2010. Postoperative pulmonary complications included those defined by the STS database.
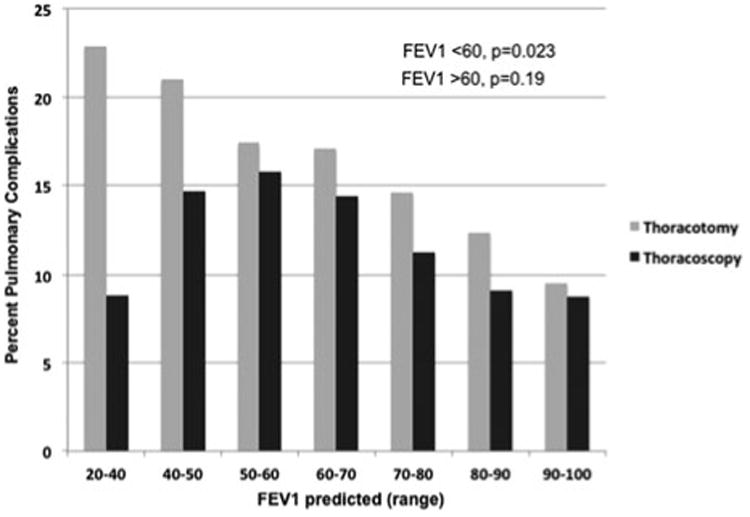
Results: In the STS database, 12,970 patients underwent lobectomy (thoracotomy, n = 8439; VATS, n = 4531) and met inclusion criteria. The overall rate of pulmonary complications was 21.7% (1832/8439) and 17.8% (806/4531) in patients undergoing lobectomy with thoracotomy and VATS, respectively (P < 0.0001). In a multivariable model of pulmonary complications, thoracotomy approach (OR = 1.25, P < 0.001), decreasing FEV1% predicted (OR = 1.01 per unit, P < 0.001) and DLCO% predicted (OR = 1.01 per unit, P < 0.001), and increasing age (1.02 per year, P < 0.001) independently predicted pulmonary complications. When examining pulmonary complications in patients with FEV1 less than 60% predicted, thoracotomy patients have markedly increased pulmonary complications when compared with VATS patients (P = 0.023). No significant difference is noted with FEV1 more than 60% predicted.
Conclusions: Poor pulmonary function predicts respiratory complications regardless of approach. Respiratory complications increase at a significantly greater rate in lobectomy patients with poor pulmonary function after thoracotomy compared with VATS. Planned surgical approach should be considered while determining whether a high-risk patient is an appropriate resection candidate.
Conflict of interest statement
Disclosure: The authors declare no conflicts of interest.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Buie VC, Owings MF, DeFrances CJ, et al. National Hospital Discharge Survey: 2006 Summary. Hy-attsville, MD: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2010. (Vital and Health Statistics, Series 13, No. 168). - PubMed
-
- McKenna RJ, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: experience with 1100 cases. Ann Thorac Surg. 2006;81:421–426. - PubMed
-
- Villamizar N, Darrabie MD, Burfeind WR, et al. Thoracoscopic lobectomy is associated with lower morbidity compared with thoracotomy. J Thorac Cardiovasc Surg. 2009;138:419–425. - PubMed
-
- Whitson BA, Groth SS, Duval SJ, et al. Surgery for early-stage non-small cell lung cancer: a systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. 2008;86:2008–2018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
