

LASIK interface complications: etiology, management, and outcomes
- PMID: 22869235
- PMCID: PMC4148820
- DOI: 10.3928/1081597X-20120722-01
LASIK interface complications: etiology, management, and outcomes
Abstract
Purpose: To describe the etiology, diagnosis, clinical course, and management of LASIK interface complications.
Methods: Literature review.
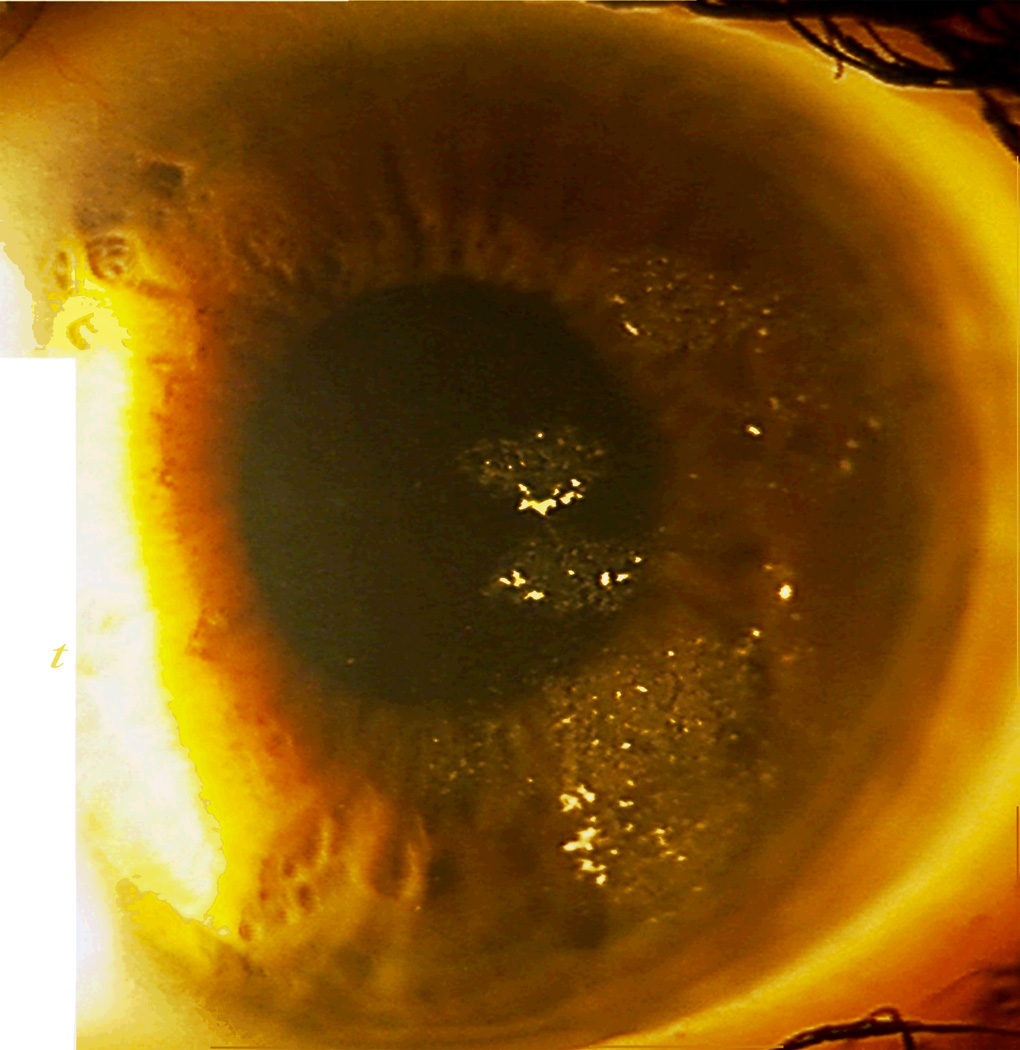
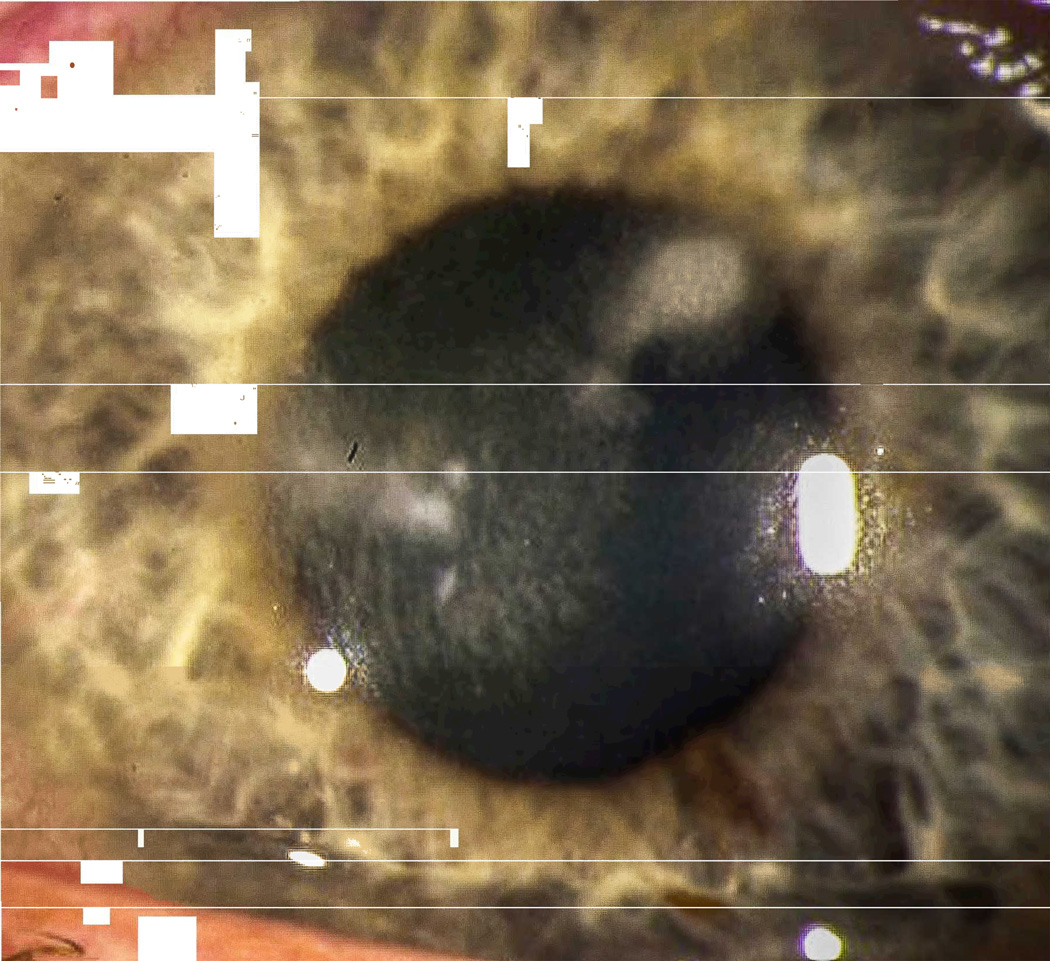
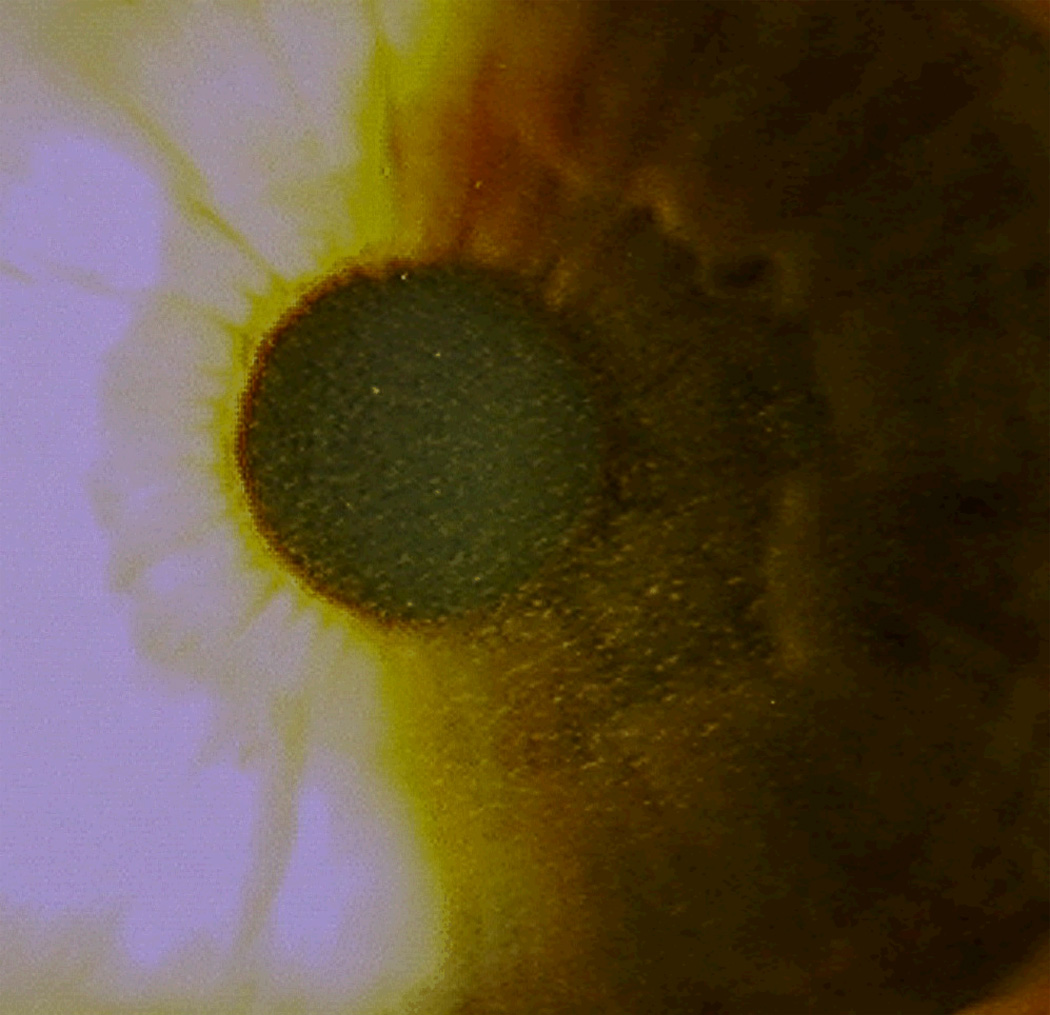
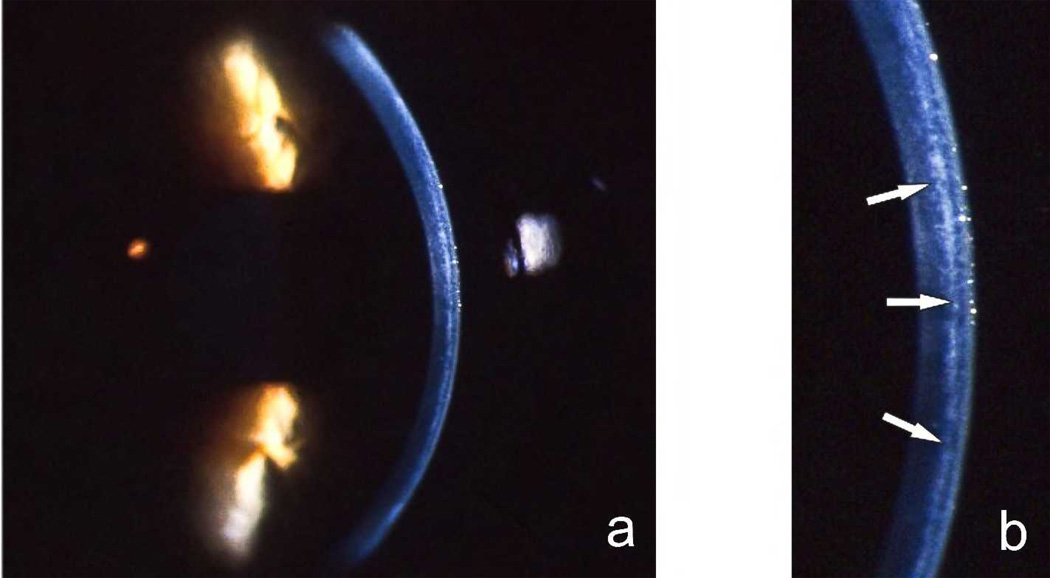
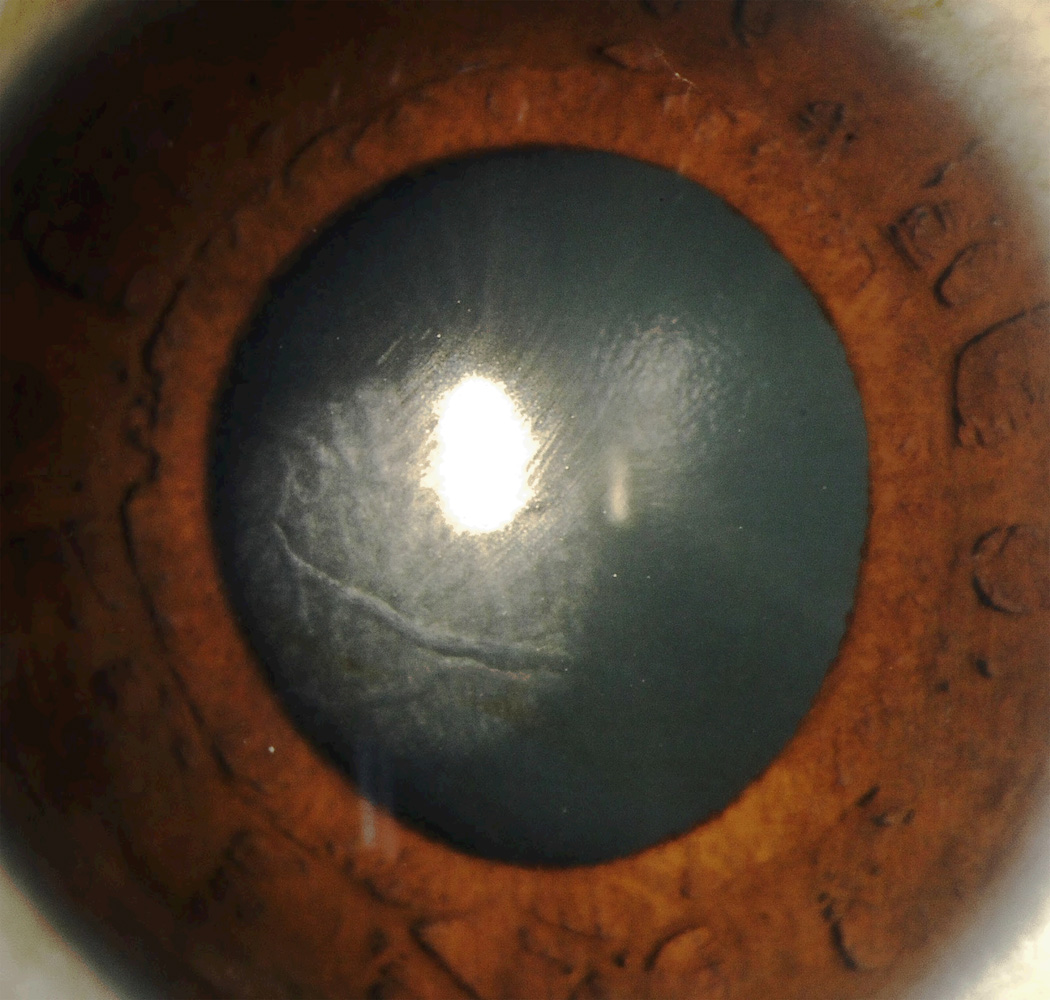
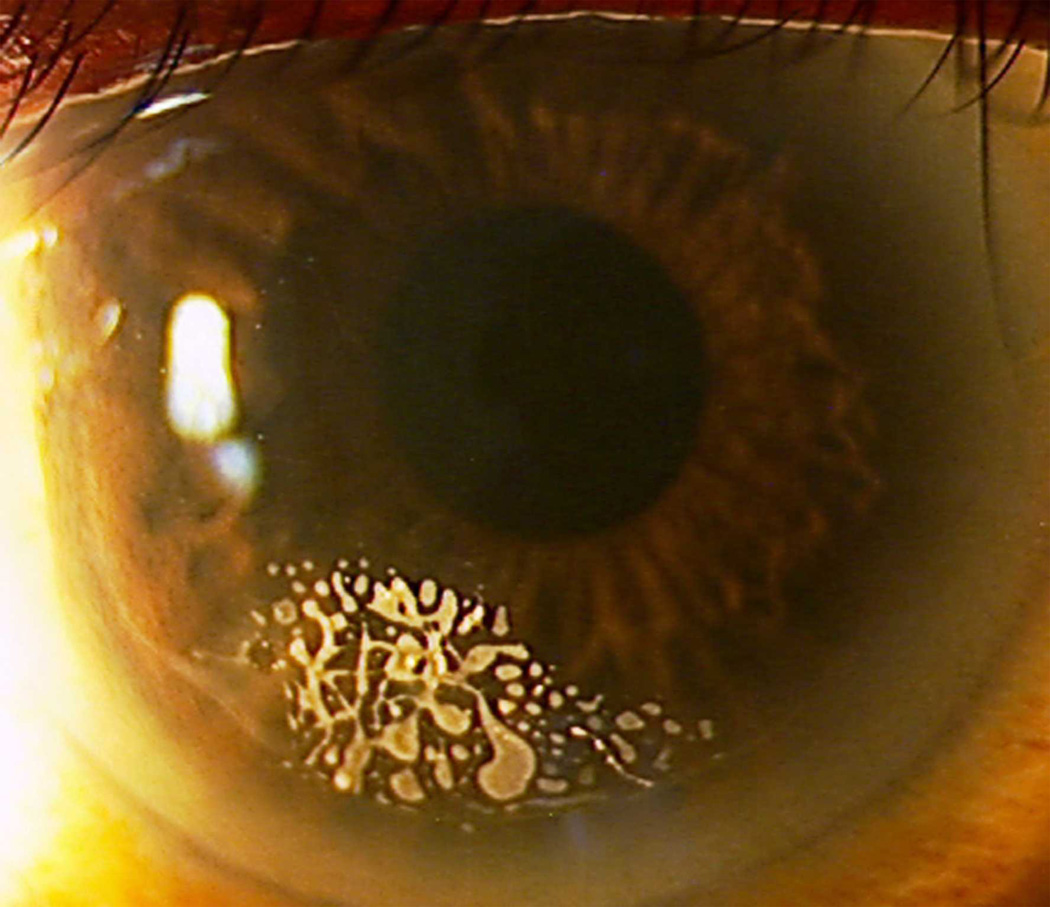
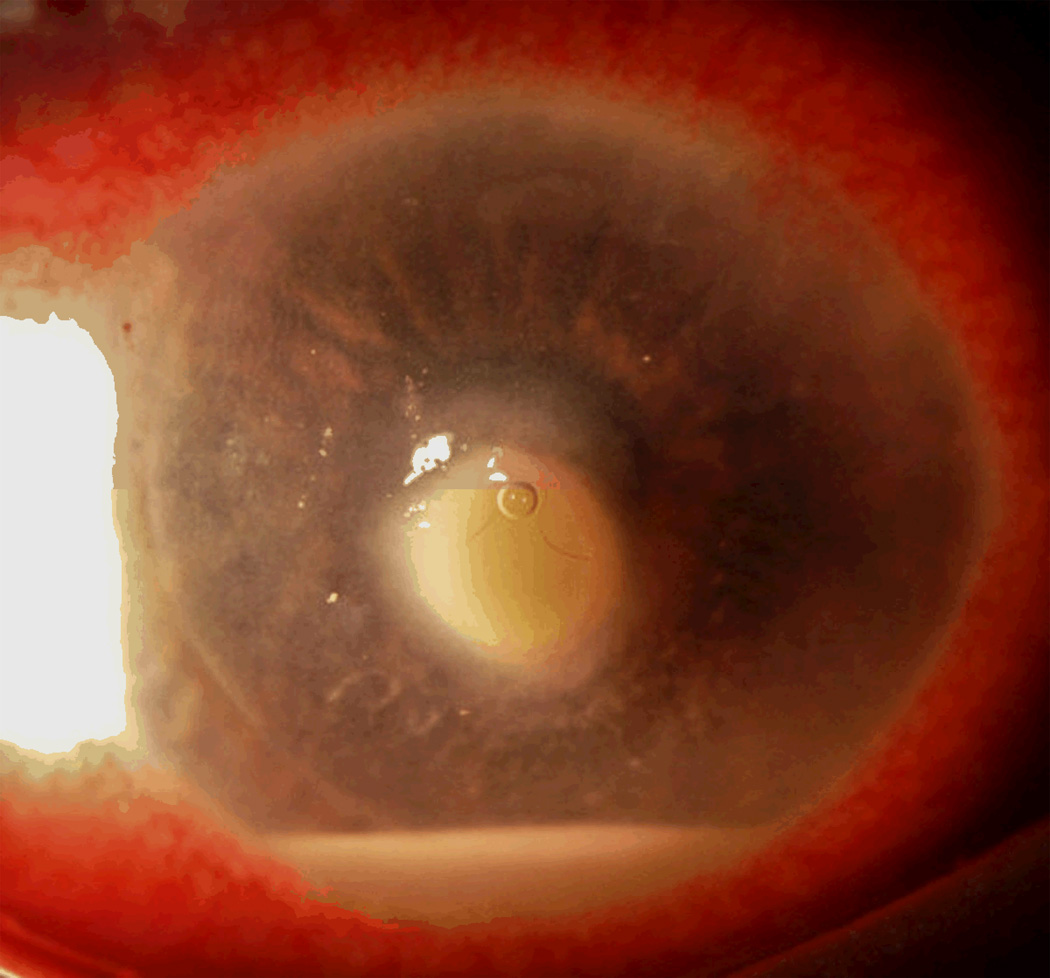
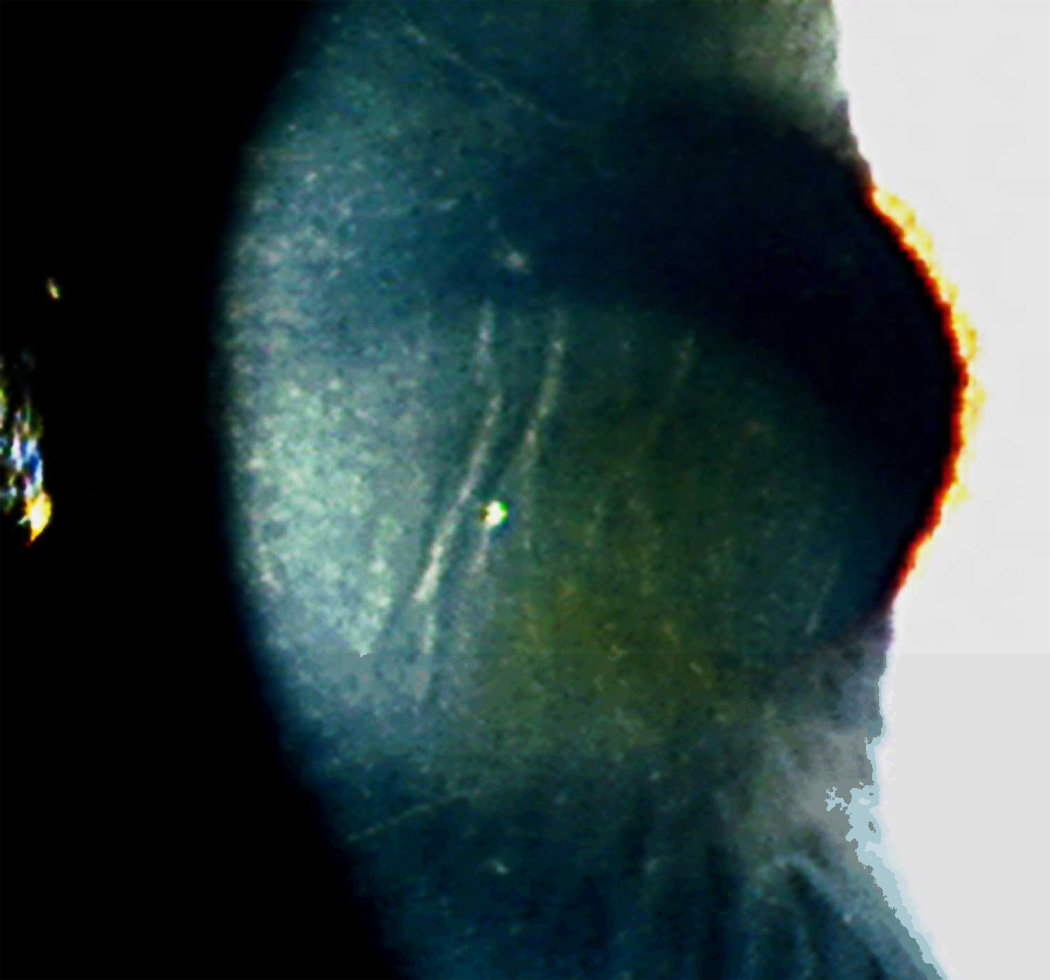
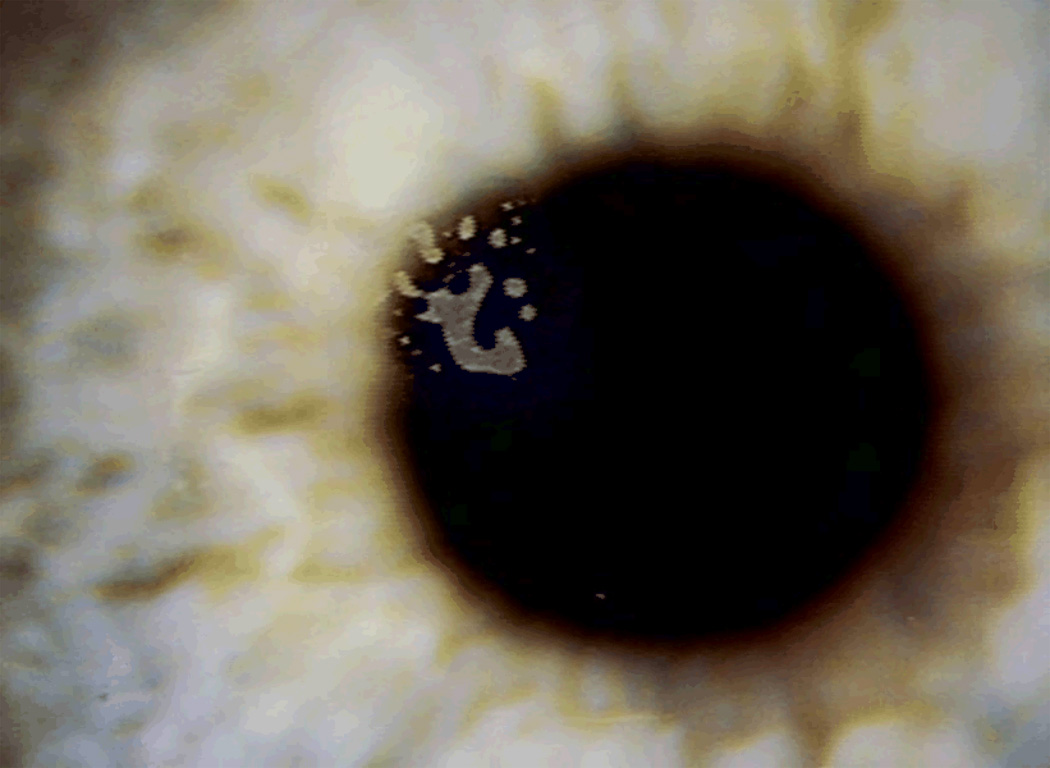
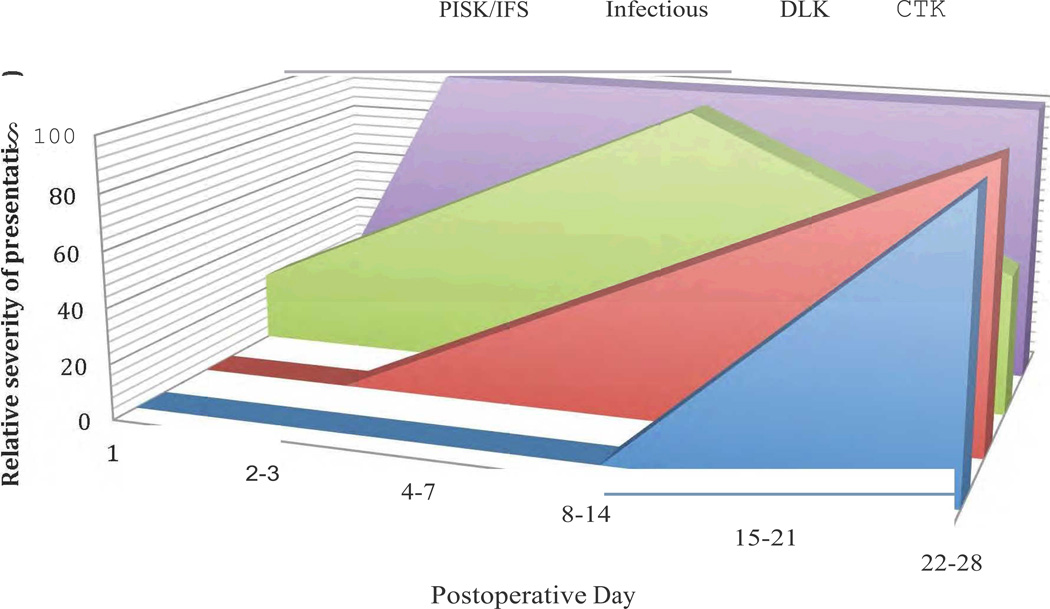
Results: Primary interface complications include infectious keratitis, diffuse lamellar keratitis, central toxic keratopathy, pressure-induced stromal keratopathy (PISK), and epithelial ingrowth. Infectious keratitis is most commonly caused by Methicillin-resistant Staphylococcus aureus (early onset) or atypical Mycobacterium (late onset) postoperatively, and immediate treatment includes flap lift and irrigation, cultures, and initiation of broad-spectrum topical antibiotics, with possible flap amputation for recalcitrant cases. Diffuse lamellar keratitis is a white blood cell infiltrate that appears within the first 5 days postoperatively and is acutely responsive to aggressive topical and oral steroid use in the early stages, but may require flap lift and irrigation to prevent flap necrosis if inflammation worsens. In contrast, PISK is caused by acute steroid response and resolves only with cessation of steroid use and intraocular pressure lowering. Without appropriate therapy PISK can result in severe optic nerve damage. Central toxic keratopathy mimics stage 4 diffuse lamellar keratitis, but occurs early in the postoperative period and is noninflammatory. Observation is the only effective treatment, and flap lift is usually not warranted. Epithelial ingrowth is easily distinguishable from other interface complications and may be self-limited or require flap lift to treat irregular astigmatism and prevent flap melt.
Conclusions: Differentiating between interface entities is critical to rapid appropriate diagnosis, treatment, and ultimate visual outcome. Although initial presentations may overlap significantly, the conditions can be readily distinguished with close follow-up, and most complications can resolve without significant visual sequelae when treated appropriately.
Copyright 2012, SLACK Incorporated.
Figures
Comment in
-
LASIK interface complications: what is the appropriate term for PISK?J Refract Surg. 2013 Feb;29(2):81. doi: 10.3928/1081597X-20130108-01. J Refract Surg. 2013. PMID: 23380406 No abstract available.
-
Pressure-induced stromal keratitis.J Refract Surg. 2013 Feb;29(2):81-2. J Refract Surg. 2013. PMID: 23479805 No abstract available.
References
-
- Dawson DG, Kramer TR, Grossniklaus HE, Waring GO, 3rd, Edelhauser HF. Histologic, ultrastructural, and immunofluorescent evaluation of human laser-assisted in situ keratomileusis corneal wounds. Archives of ophthalmology. 2005;123:741–756. - PubMed
-
- Llovet F, de Rojas V, Interlandi E, et al. Infectious keratitis in 204 586 LASIK procedures. Ophthalmology. 2010;117:232–238. e1–e4. - PubMed
-
- Stulting RD, Randleman JB, Couser JM, Thompson KP. The epidemiology of diffuse lamellar keratitis. Cornea. 2004;23:680–688. - PubMed
-
- Chang MA, Jain S, Azar DT. Infections following laser in situ keratomileusis: an integration of the published literature. Survey of ophthalmology. 2004;49:269–280. - PubMed
-
- Donnenfeld ED, Kim T, Holland EJ, et al. ASCRS White Paper: Management of infectious keratitis following laser in situ keratomileusis. Journal of cataract and refractive surgery. 2005;31:2008–2011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
