

Comparative study of laparoscopy-assisted versus open subtotal gastrectomy for pT2 gastric cancer
- PMID: 22869478
- PMCID: PMC3423848
- DOI: 10.3349/ymj.2012.53.5.952
Comparative study of laparoscopy-assisted versus open subtotal gastrectomy for pT2 gastric cancer
Abstract
Purpose: Laparoscopy-assisted distal gastrectomy (LADG) is a widely accepted surgery for early gastric cancer. However, its use in advanced gastric cancer has rarely been studied. The aim of this study is to investigate the feasibility and survival outcomes of LADG for pT2 gastric cancer.
Materials and methods: Between January 2004 and December 2009, we evaluated 67 and 52 patients who underwent open distal gastrectomy (ODG) and LADG, respectively, with diagnosis of pT2 gastric cancer. The clinicopathological characteristics, postoperative outcomes, and survival were retrospectively compared between the two groups.
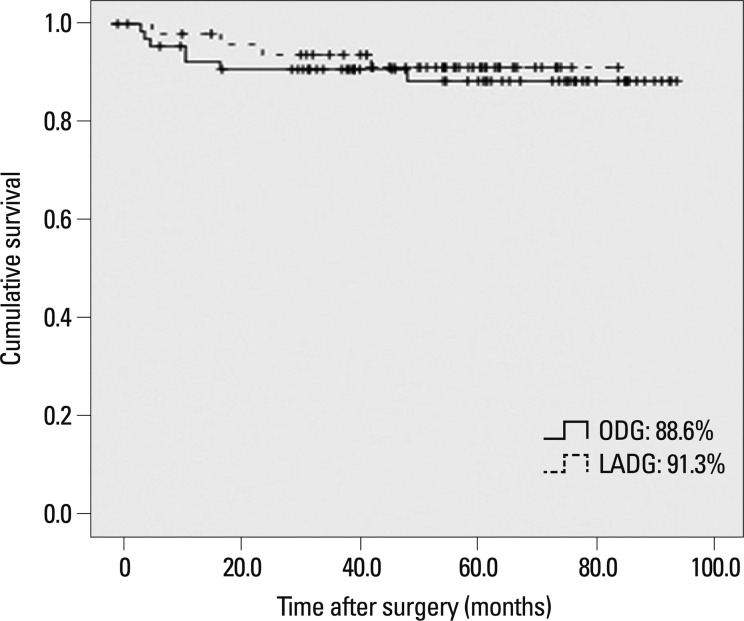
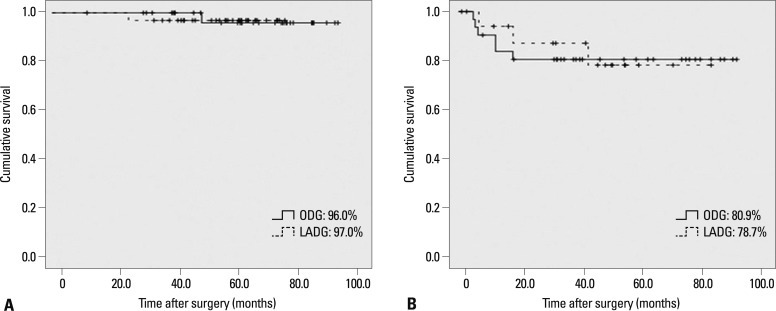
Results: There were statistically significant differences in the proximal margin of the clinicopathological parameters. The operation time was significantly longer in LADG than in ODG (207.7 vs. 159.9 minutes). There were 6 (9.0%) and 5 (9.6%) complications in ODG and LADG, respectively. During follow-up periods, tumor recurrence occurred in 7 (10.4%) patients of the ODG and in 4 (7.7%) patients of the LADG group. The 5-year survival rate of ODG and LADG was 88.6% and 91.3% (p=0.613), respectively. In view of lymph node involvement, 5-year survival rates were 96.0% in ODG versus 97.0% in LADG for patients with negative nodal metastasis (p=0.968) and 80.9% in ODG versus 78.7% in LADG for those with positive nodal metastasis (p=0.868).
Conclusion: Although prospective study is necessary to compare LADG with open gastrectomy for the treatment of advanced gastric cancer, laparoscopy-assisted distal gastrectomy might be considered as an alternative treatment for some pT2 gastric cancer.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Comparison of outcomes for laparoscopically assisted and open radical distal gastrectomy with lymphadenectomy for advanced gastric cancer.Surg Endosc. 2011 Sep;25(9):2960-6. doi: 10.1007/s00464-011-1652-y. Epub 2011 Apr 22. Surg Endosc. 2011. PMID: 21512884
-
Laparoscopy-assisted versus open distal gastrectomy for gastric cancer in elderly patients: a retrospective comparative study.Surg Endosc. 2016 Sep;30(9):4069-77. doi: 10.1007/s00464-015-4722-8. Epub 2015 Dec 29. Surg Endosc. 2016. PMID: 26715017
-
Laparoscopy-assisted versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: Results From a Randomized Phase II Multicenter Clinical Trial (COACT 1001).Ann Surg. 2018 Apr;267(4):638-645. doi: 10.1097/SLA.0000000000002168. Ann Surg. 2018. PMID: 28187041 Clinical Trial.
-
Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: A meta-analysis based on seven randomized controlled trials.Surg Oncol. 2015 Jun;24(2):71-7. doi: 10.1016/j.suronc.2015.02.003. Epub 2015 Mar 5. Surg Oncol. 2015. PMID: 25791201 Review.
-
Comparison of laparoscopy-assisted by conventional open distal gastrectomy and extraperigastric lymph node dissection in early gastric cancer.J Surg Oncol. 2005 Jul 1;91(1):90-4. doi: 10.1002/jso.20271. J Surg Oncol. 2005. PMID: 15999352 Review.
Cited by
-
Comparison of estimated treatment effects between randomized controlled trials, case-matched, and cohort studies on laparoscopic versus open distal gastrectomy for advanced gastric cancer: a systematic review and meta-analysis.Langenbecks Arch Surg. 2022 Jun;407(4):1381-1397. doi: 10.1007/s00423-022-02454-3. Epub 2022 Feb 3. Langenbecks Arch Surg. 2022. PMID: 35113227
-
Laparoscopic versus open approach in gastrectomy for advanced gastric cancer: a systematic review.World J Surg Oncol. 2020 Jun 13;18(1):126. doi: 10.1186/s12957-020-01888-7. World J Surg Oncol. 2020. PMID: 32534587 Free PMC article.
-
Short-term surgical outcomes of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer.Surg Endosc. 2018 May;32(5):2427-2433. doi: 10.1007/s00464-017-5942-x. Epub 2017 Dec 12. Surg Endosc. 2018. PMID: 29234941 Clinical Trial.
-
Oncologic value of laparoscopy-assisted distal gastrectomy for advanced gastric cancer: A systematic review and meta-analysis.J Minim Access Surg. 2016 Jul-Sep;12(3):199-208. doi: 10.4103/0972-9941.181283. J Minim Access Surg. 2016. PMID: 27279389 Free PMC article. Review.
-
Long-term survival outcomes of laparoscopic versus open gastrectomy for gastric cancer: a systematic review and meta-analysis.Medicine (Baltimore). 2015 Jan;94(4):e454. doi: 10.1097/MD.0000000000000454. Medicine (Baltimore). 2015. PMID: 25634185 Free PMC article.
References
-
- Ohtsu A, Yoshida S, Saijo N. Disparities in gastric cancer chemotherapy between the East and West. J Clin Oncol. 2006;24:2188–2196. - PubMed
-
- Adachi Y, Shiraishi N, Kitano S. Modern treatment of early gastric cancer: review of the Japanese experience. Dig Surg. 2002;19:333–339. - PubMed
-
- Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4:146–148. - PubMed
-
- Kim MC, Kim KH, Kim HH, Jung GJ. Comparison of laparoscopy-assisted by conventional open distal gastrectomy and extraperigastric lymph node dissection in early gastric cancer. J Surg Oncol. 2005;91:90–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
