

Development of the rectus abdominis and its sheath in the human fetus
- PMID: 22869489
- PMCID: PMC3423835
- DOI: 10.3349/ymj.2012.53.5.1028
Development of the rectus abdominis and its sheath in the human fetus
Abstract
Purpose: Although the rectus abdominis and its sheath are well known structures, their development in the human fetus is poorly understood.
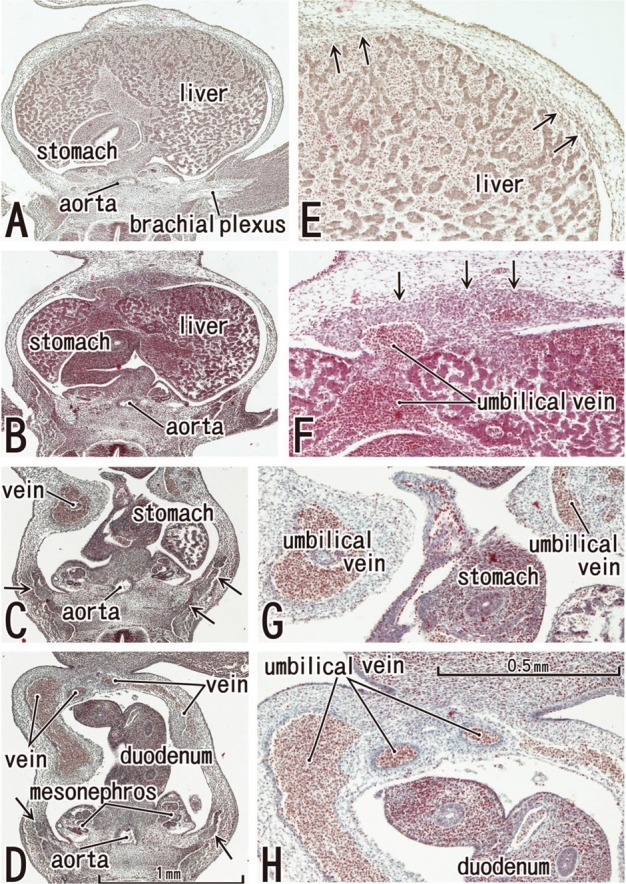
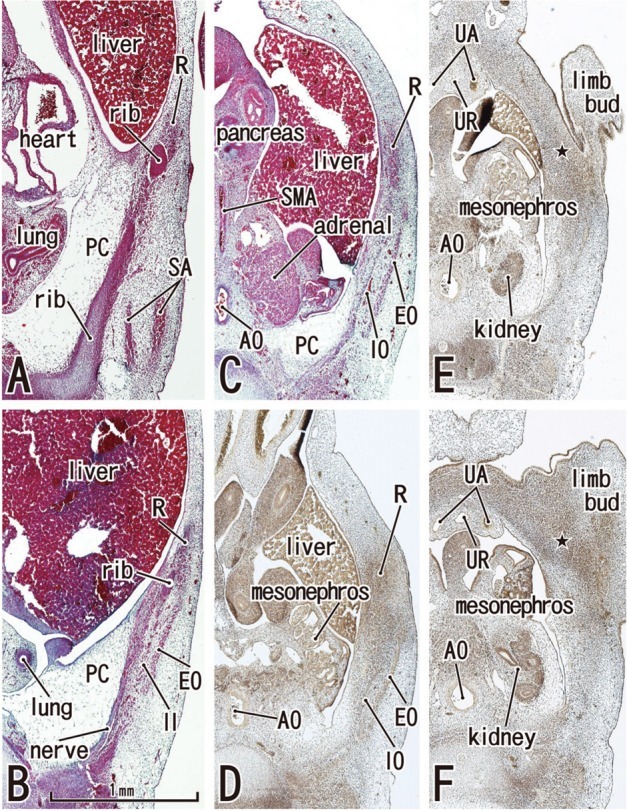
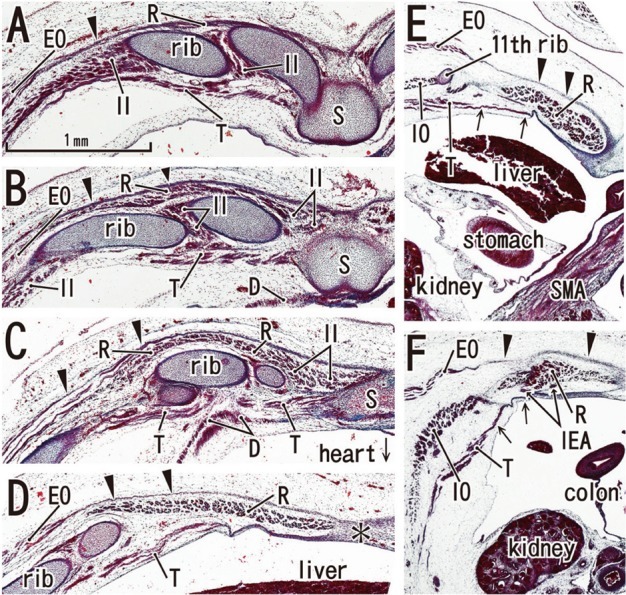
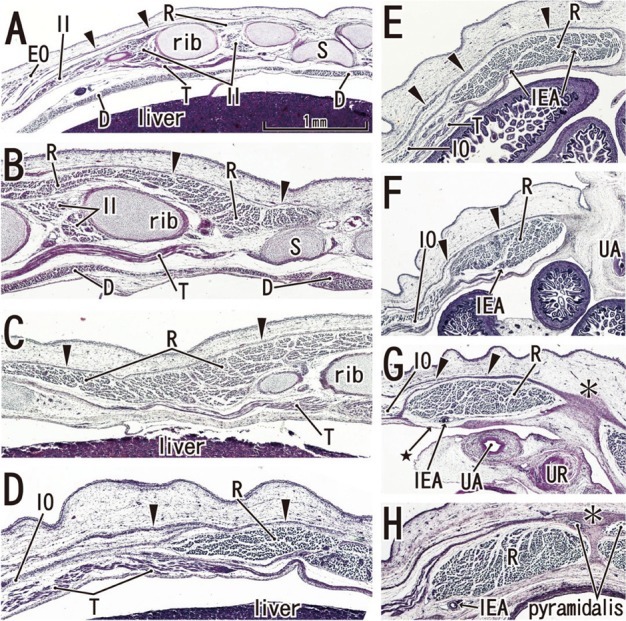
Materials and methods: We examined rectus abdominis and sheath development in semiserial horizontal sections of 18 fetuses at 5-9 weeks of gestation.
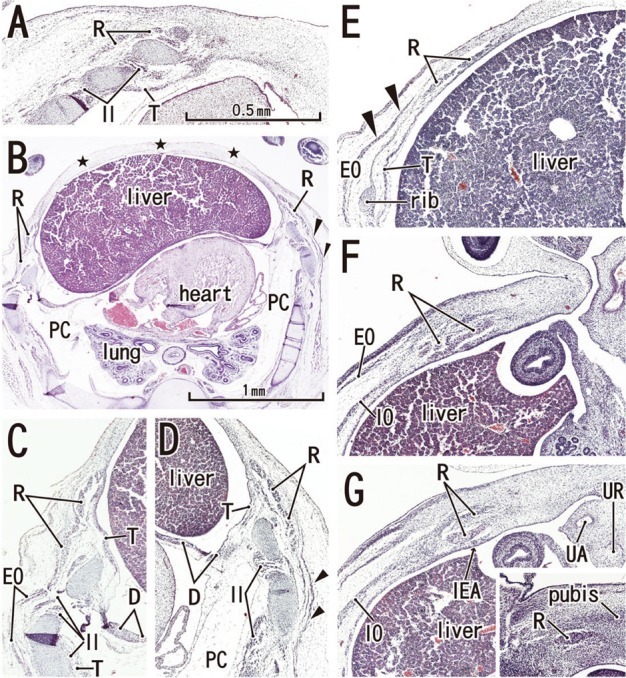
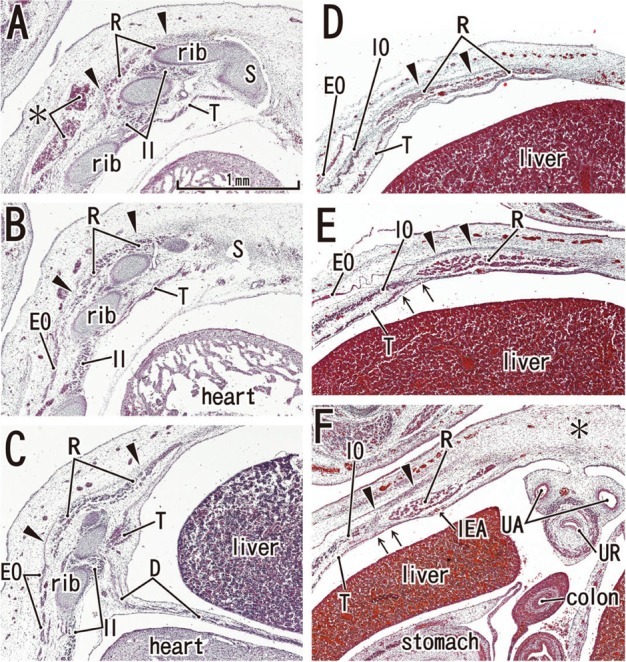
Results: Rectus muscle differentiation was found to commence above the umbilicus at 6 weeks and extend inferiorly. Until closure of the anterior chest wall via fusion of the bilateral sternal anlagen (at 7 weeks), the anterior rectal sheath originated from the external oblique and developed towards the medial margin of the rectus abdominis at all levels, including the supracostal part. After formation of the anterior sheath, fascial laminae from the internal oblique and transversus abdominis contributed to formation of the posterior rectus sheath. However, the posterior sheath was absent along the supracostal part of the rectus abdominis, as the transversus muscle fibers reached the sternum or the midline area. Therefore, it appeared that resolution of the physiological umbilical hernia (8-9 weeks) as well as chest wall closure was not required for development of the rectus abdominis and its sheath. Conversely, in the inferior part of the two largest fetal specimens, after resolution of the hernia, the posterior sheath underwent secondary disappearance, possibly due to changes in mechanical stress.
Conclusion: Upward extension of the rectus abdominis suddenly stopped at the margin of the inferiorly developing pectoralis major without facing the external intercostalis. The rectus thoracis, if present, might correspond to the pectoralis.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Williams PL. Gray's Anatomy. 38th ed. Edinburgh: Churchill Livingstone; 1995. pp. 825–829.
-
- Munger GT, Munger BL. Differentiation of the anterior body wall and truncal epidermis and associated co-migration of cutaneous nerves and mesenchyme. Anat Rec. 1991;231:261–274. - PubMed
-
- Gościcka D, Murawski E. Tendinous intersections of the rectus abdominis muscle in human fetuses. Folia Morphol (Warsz) 1980;39:427–434. - PubMed
-
- Niikura H, Okamoto S, Nagase S, Takano T, Murakami G, Tatsumi H, et al. Fetal development of the human gubernaculum with special reference to the fasciae and muscles around it. Clin Anat. 2008;21:547–557. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
