

Quantifying pulmonary regurgitation and right ventricular function in surgically repaired tetralogy of Fallot: a comparative analysis of echocardiography and magnetic resonance imaging
- PMID: 22869820
- PMCID: PMC3476467
- DOI: 10.1161/CIRCIMAGING.112.972588
Quantifying pulmonary regurgitation and right ventricular function in surgically repaired tetralogy of Fallot: a comparative analysis of echocardiography and magnetic resonance imaging
Abstract
Background: Patients with repaired tetralogy of Fallot are monitored for pulmonary regurgitation (PR) and right ventricular (RV) function. We sought to compare measures of PR and RV function on echocardiogram to those on cardiac magnetic resonance (CMR) and to develop a new tool for assessing PR by echocardiogram.
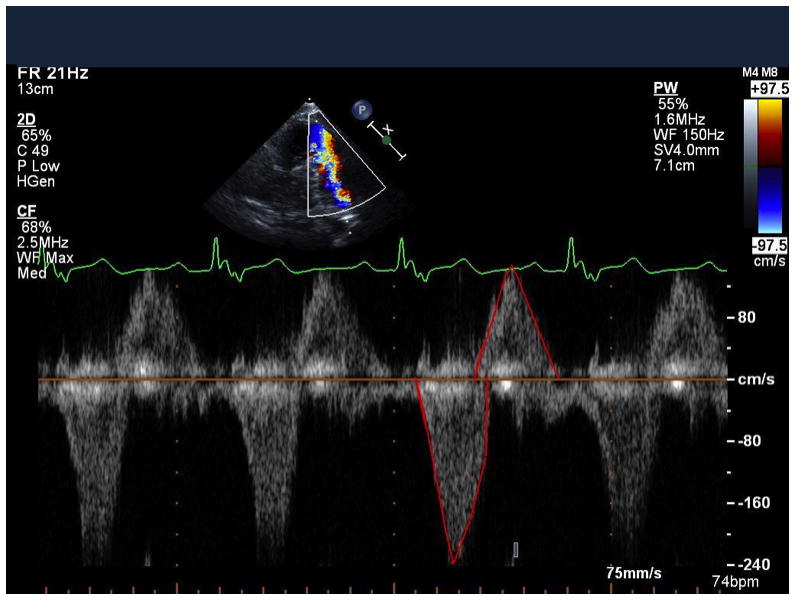
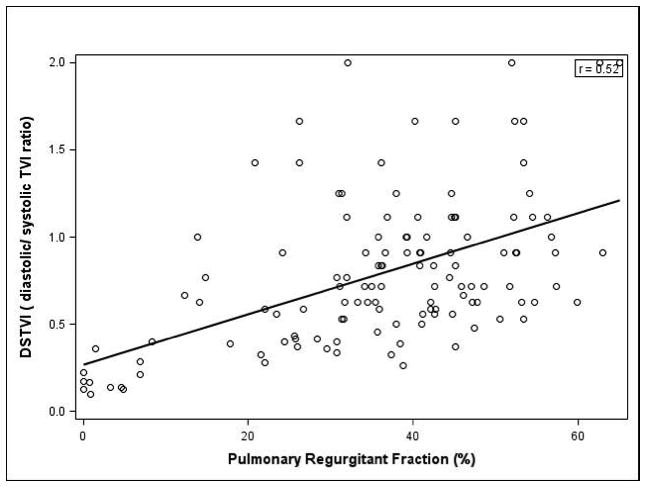
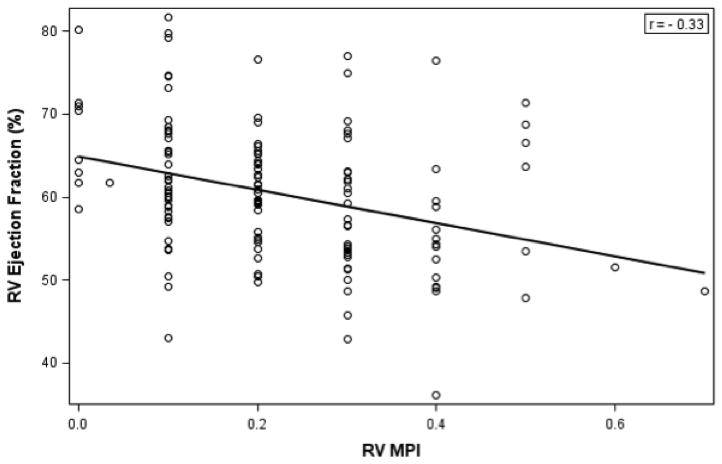
Methods and results: Patients with repaired tetralogy of Fallot (n=143; 12.5±3.2 years) had an echocardiogram and CMR within 3 months of each other. On echocardiogram, RV function was assessed by (1) Doppler tissue imaging of the RV free wall and (2) myocardial performance index. The ratio of diastolic and systolic time-velocity integrals measured by Doppler of the main pulmonary artery was calculated. CMR variables included RV ejection fraction, RV volumes, and pulmonary regurgitant fraction (RF). Pulmonary regurgitation was graded as mild (RF<20%), moderate (RF=20-40%), and severe (RF>40%). On CMR, RF was 34+17% and RV ejection fraction was 61+8%. Echocardiography had good sensitivity identifying cases with RF>20% (sensitivity 97%; 95% CI: 92-99%) but overestimated the amount of PR when RF<20% (false-positive rate 36%; 95% CI: 18-57%). The diastolic and systolic time-velocity integrals on echocardiogram showed moderate correlation with RF on CMR (R=0.60; P<0.0001). On CMR, RF of 20% and 40% corresponded with a diastolic and systolic time-velocity integral of 0.49 (95% CI: 0.44-0.56) and 0.72 (95% CI: 0.68-0.76), respectively. RV myocardial performance index correlated modestly with RV ejection fraction (r=-0.33; P<0.001).
Conclusions: This study suggests that the diastolic and systolic time-velocity integrals ratio may make a modest contribution to the overall assessment of PR in patients with repaired tetralogy of Fallot and warrants further investigation. However, echocardiography continues to have a limited ability to quantify PR and RV function as compared with CMR.
Figures
References
-
- Murphy JG, Gersh BJ, Mair DD, Fuster V, McGoon MD, Ilstrup DM, McGoon DC, Kirklin JW, Danielson GK. Long-term outcome in patients undergoing surgical repair of tetralogy of fallot. N Engl J Med. 1993;329:593–599. - PubMed
-
- Nollert G, Fischlein T, Bouterwek S, Bohmer C, Klinner W, Reichart B. Long-term survival in patients with repair of tetralogy of fallot: 36-year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol. 1997;30:1374–1383. - PubMed
-
- Hickey EJ, Veldtman G, Bradley TJ, Gengsakul A, Manlhiot C, Williams WG, Webb GD, McCrindle BW. Late risk of outcomes for adults with repaired tetralogy of fallot from an inception cohort spanning four decades. Eur J Cardiothorac Surg. 2009;35:156–164. - PubMed
-
- Bacha EA, Scheule AM, Zurakowski D, Erickson LC, Hung J, Lang P, Mayer JE, Jr, del Nido PJ, Jonas RA. Long-term results after early primary repair of tetralogy of fallot. J Thorac Cardiovasc Surg. 2001;122:154–161. - PubMed
-
- Gatzoulis MA, Balaji S, Webber SA, Siu SC, Hokanson JS, Poile C, Rosenthal M, Nakazawa M, Moller JH, Gillette PC, Webb GD, Redington AN. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of fallot: A multicentre study. Lancet. 2000;356:975–981. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
