

Approach to the patient with anaplastic thyroid carcinoma
- PMID: 22869844
- PMCID: PMC3410281
- DOI: 10.1210/jc.2012-1314
Approach to the patient with anaplastic thyroid carcinoma
Abstract
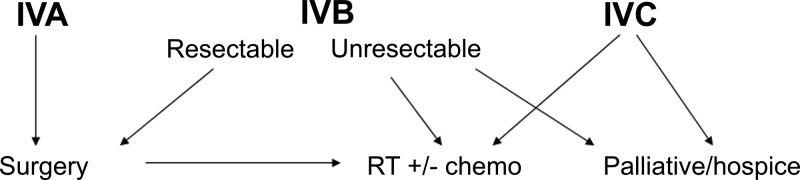
Anaplastic thyroid carcinoma is the least common but most lethal of thyroid cancers. All patients are classified as stage IV, with the primary lesion restricted to the thyroid gland in stage IVA; locoregional lymph nodes may exist in IVA/IVB; and IVC disease is defined by distant metastases. Prognosis is highly dependent on disease extent at presentation, and staging and establishing a plan of care must be accomplished quickly. Although almost all studies are biased due to their retrospective nature, the most important factors associated with longer survival are completeness of surgical resection (achievable in only a minority of patients) and high-dose (>40 Gy) external beam radiotherapy (preferably intensity modulated radiation therapy). Recent reports suggest that a multimodal approach (surgery, radiation, and chemotherapy) is beneficial. Given the high lethality even with apparent local disease, combination systemic therapy (cytotoxics and/or targeted agents) may improve outcomes in stage IVA/IVB patients. Newer, more effective drug combinations are urgently needed for IVC patients who want aggressive therapy. A candid discussion of the prognosis and management options, including palliative care/hospice, should be held with the patient and caregiver as soon as possible after diagnosis to clarify the patient's preference and expectations. Prospective multicenter clinical trials, incorporating molecular analyses of tumors, are required if we are to improve survival in anaplastic thyroid carcinoma.
Figures

References
-
- Siegel R, Ward E, Brawley O, Jemal A. 2011. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 61:212–236 - PubMed
-
- Al-Hamdan N, Ravichandran K, Al-Sayyad J, Al-Lawati J, Khazal Z, Al-Khateeb F, Abdulwahab A, Al-Asfour A. 2009. Incidence of cancer in Gulf Cooperation Council countries, 1998–2001. East Mediterr Health J 15:600–611 - PubMed
-
- Smallridge RC, Abate E, Anaplastic thyroid carcinoma: clinical aspects. In: Wartofsky L, Van Nostrand D, eds. Thyroid cancer: a comprehensive guide to clinical management. 3rd ed (in press) New York: Springer
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
