

Impact of community tracer teams on treatment outcomes among tuberculosis patients in South Africa
- PMID: 22871071
- PMCID: PMC3490985
- DOI: 10.1186/1471-2458-12-621
Impact of community tracer teams on treatment outcomes among tuberculosis patients in South Africa
Abstract
Background: Tuberculosis (TB) indicators in South Africa currently remain well below global targets. In 2008, the National Tuberculosis Program (NTP) implemented a community mobilization program in all nine provinces to trace TB patients that had missed a treatment or clinic visit. Implementation sites were selected by TB program managers and teams liaised with health facilities to identify patients for tracing activities. The objective of this analysis was to assess the impact of the TB Tracer Project on treatment outcomes among TB patients.
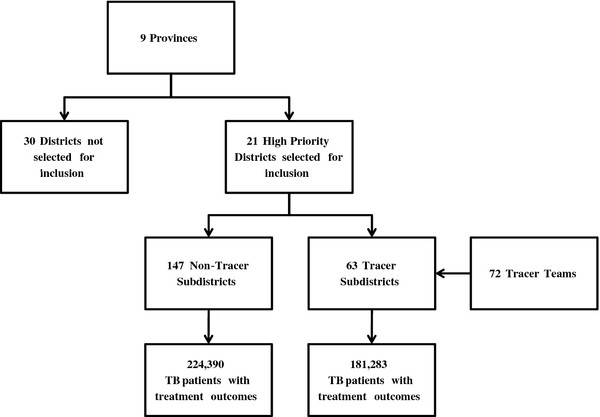
Methods: The study population included all smear positive TB patients registered in the Electronic TB Registry from Quarter 1 2007-Quarter 1 2009 in South Africa. Subdistricts were used as the unit of analysis, with each designated as either tracer (standard TB program plus tracer project) or non-tracer (standard TB program only). Mixed linear regression models were utilized to calculate the percent quarterly change in treatment outcomes and to compare changes in treatment outcomes from Quarter 1 2007 to Quarter 1 2009 between tracer and non-tracer subdistricts.
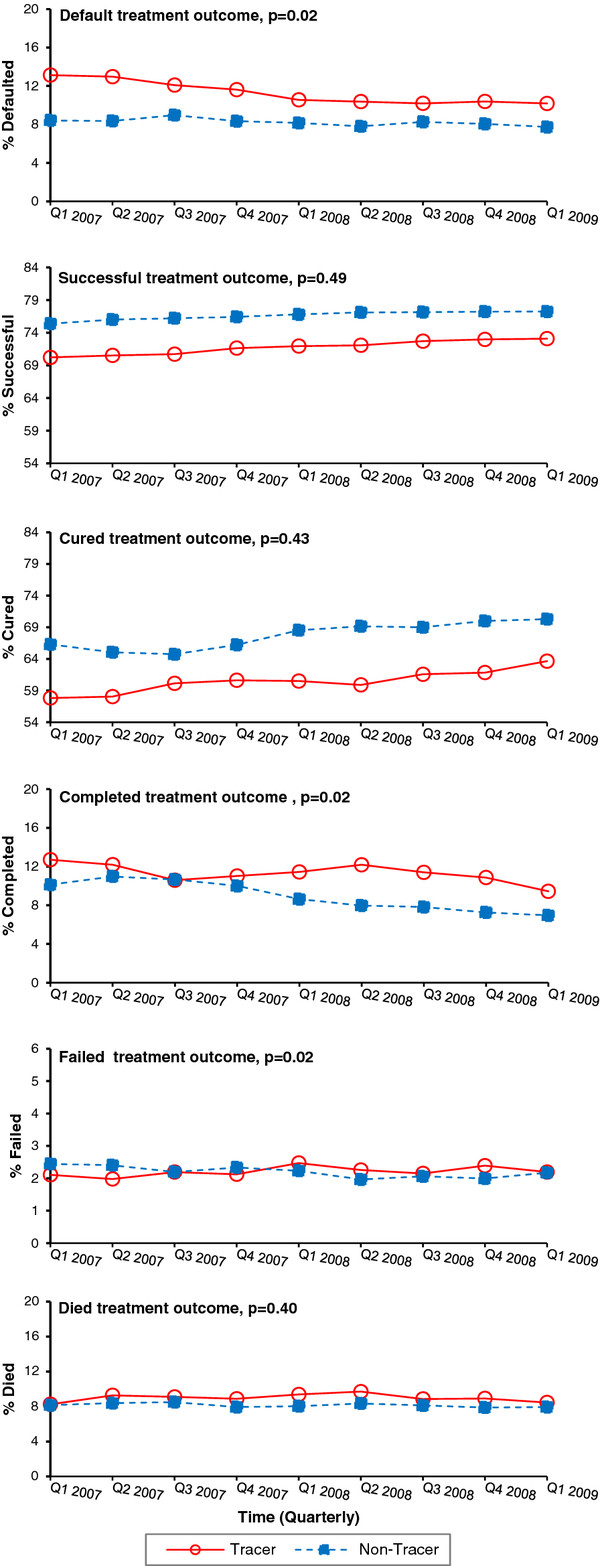
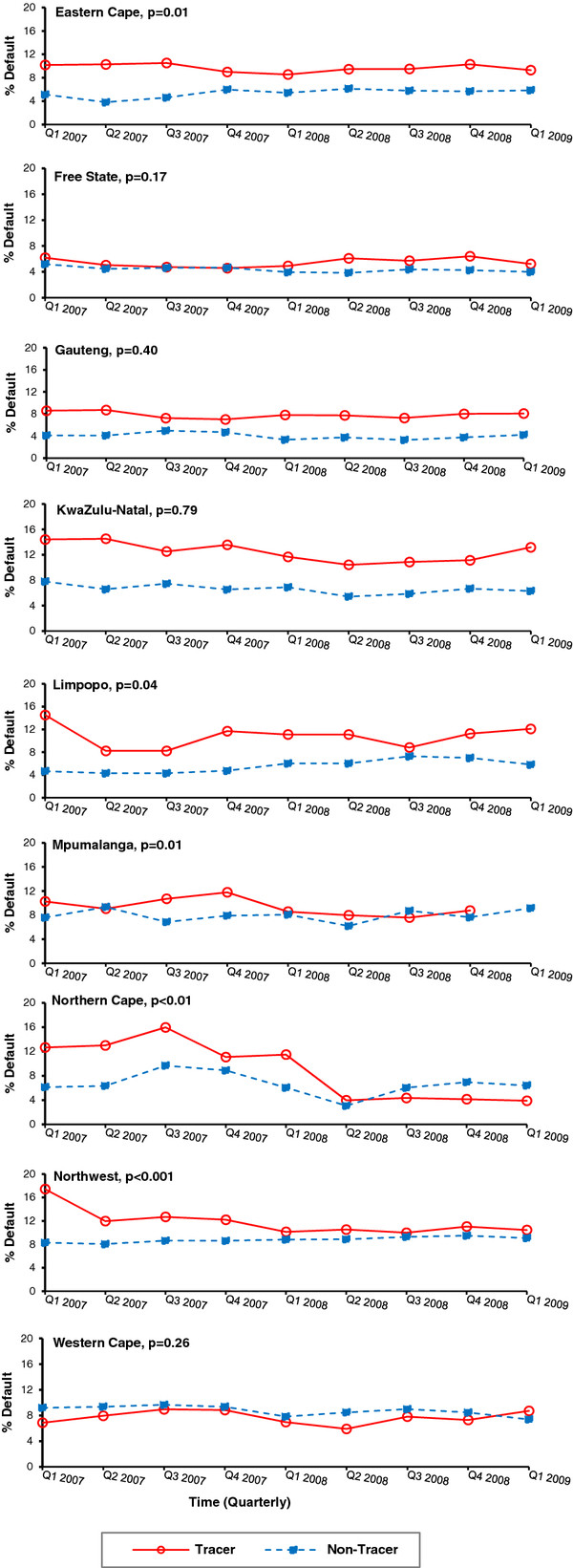
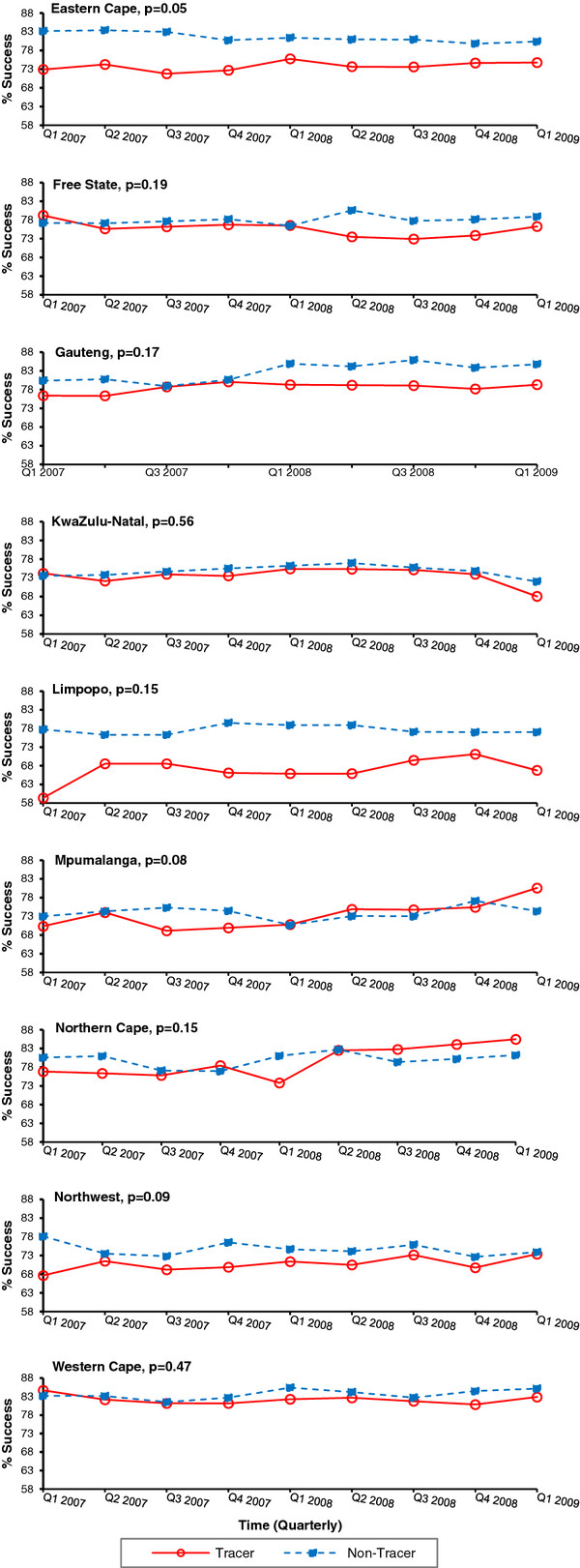
Results: For all provinces combined, the percent quarterly change decreased significantly for default treatment outcomes among tracer subdistricts (-0.031%; p < 0.001) and increased significantly for successful treatment outcomes among tracer subdistricts (0.003%; p = 0.03). A significant decrease in the proportion of patient default was observed for all provinces combined over the time period comparing tracer and non-tracer subdistricts (p = 0.02). Examination in stratified models revealed the results were not consistent across all provinces; significant differences were observed between tracer and non-tracer subdistricts over time in five of nine provinces for treatment default.
Conclusions: Community mobilization of teams to trace TB patients that missed a clinic appointment or treatment dose may be an effective strategy to mitigate default rates and improve treatment outcomes. Additional information is necessary to identify best practices and elucidate discrepancies across provinces; these findings will help guide the NTP in optimizing the adoption of tracing activities for TB control.
Figures
References
-
- World Health Organization. Global tuberculosis control: WHO Report 2010. Geneva Switzerland: WHO; 2010.
-
- Health SANDo. Draft National Tuberculosis Policy Guidelines 2008. Pretoria, South Africa: National Department of Health of the Republic of South Africa; 2008. The National Tuberculosis Control Programme.
-
- World Health Organization. WHO Report 2008: Global tuberculosis control - epidemiology, strategy, financing. Geneva Switzerland: WHO; 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
