

Effects of sildenafil and/or muscle derived stem cells on myocardial infarction
- PMID: 22871104
- PMCID: PMC3476974
- DOI: 10.1186/1479-5876-10-159
Effects of sildenafil and/or muscle derived stem cells on myocardial infarction
Abstract
Background: Previous studies have shown that long-term oral daily PDE 5 inhibitors (PDE5i) counteract fibrosis, cell loss, and the resulting dysfunction in tissues of various rat organs and that implantation of skeletal muscle-derived stem cells (MDSC) exerts some of these effects. PDE5i and stem cells in combination were found to be more effective in non-MI cardiac repair than each treatment separately. We have now investigated whether sildenafil at lower doses and MDSC, alone or in combination are effective to attenuate LV remodeling after MI in rats.
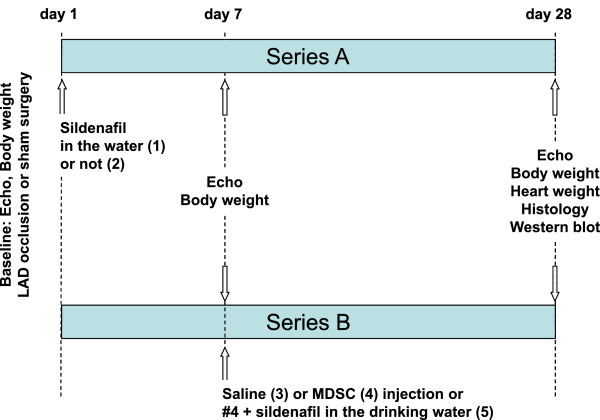
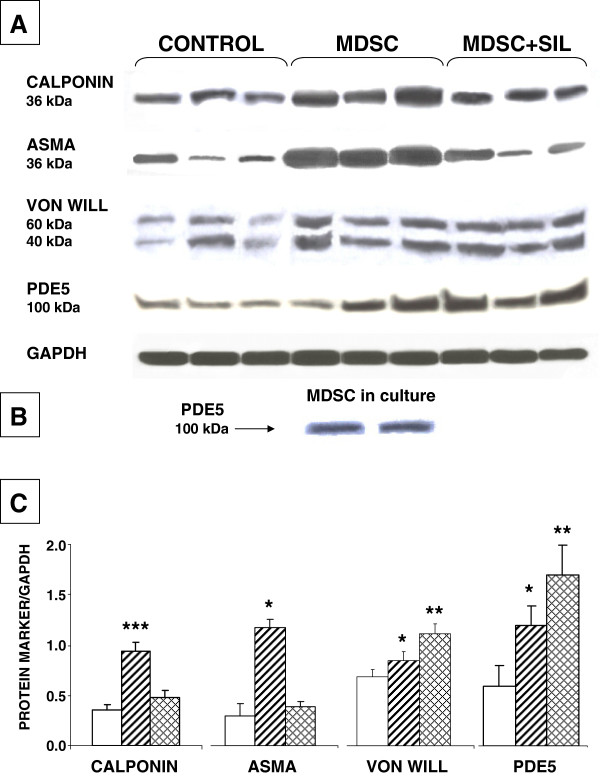
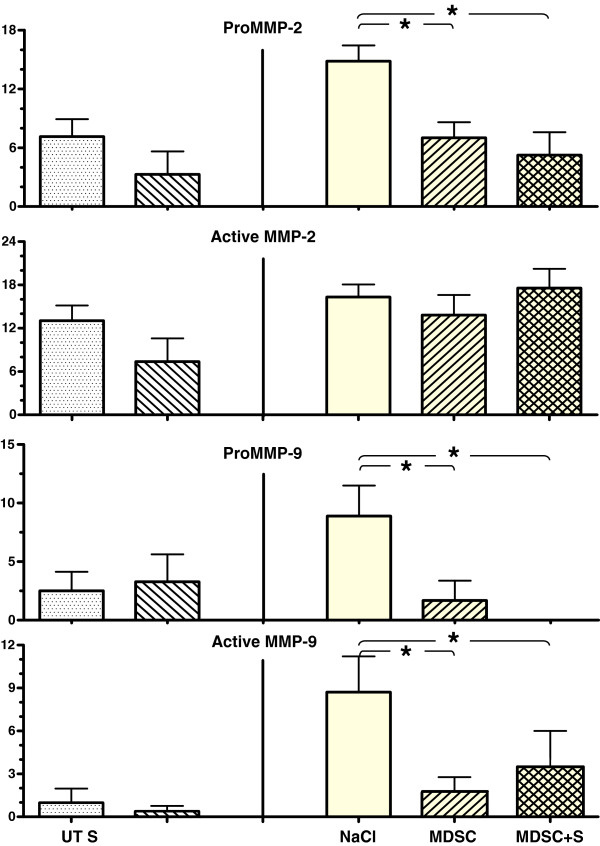
Methods: MI was induced in rats by ligature of the left anterior descending coronary artery. Treatment groups were: "Series A": 1) untreated; 2) oral sildenafil 3 mg/kg/day from day 1; and "Series B": intracardiac injection at day 7 of: 3) saline; 4) rat MDSC (106 cells); 5) as #4, with sildenafil as in #2. Before surgery, and at 1 and 4 weeks, the left ventricle ejection fraction (LVEF) was measured. LV sections were stained for collagen, myofibroblasts, apoptosis, cardiomyocytes, and iNOS, followed by quantitative image analysis. Western blots estimated angiogenesis and myofibroblast accumulation, as well as potential sildenafil tachyphylaxis by PDE 5 expression. Zymography estimated MMPs 2 and 9 in serum.
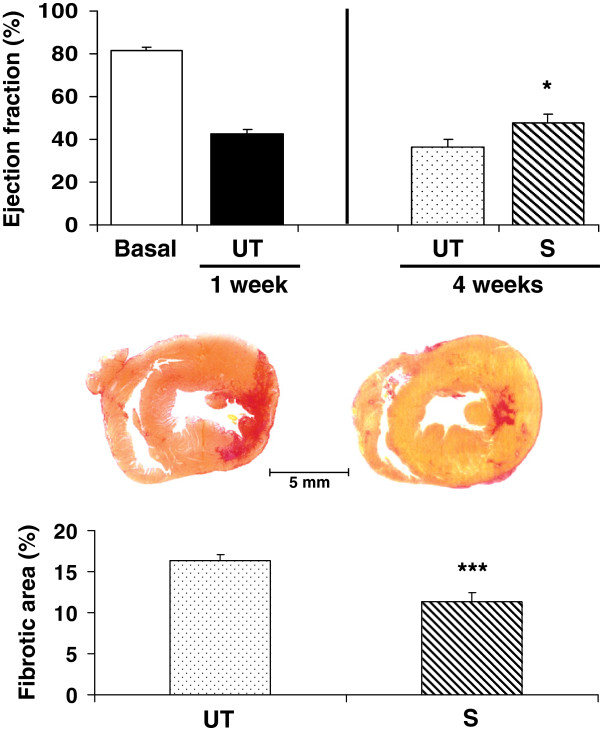
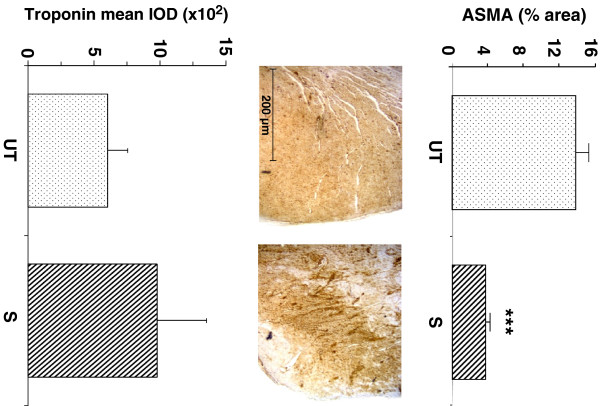
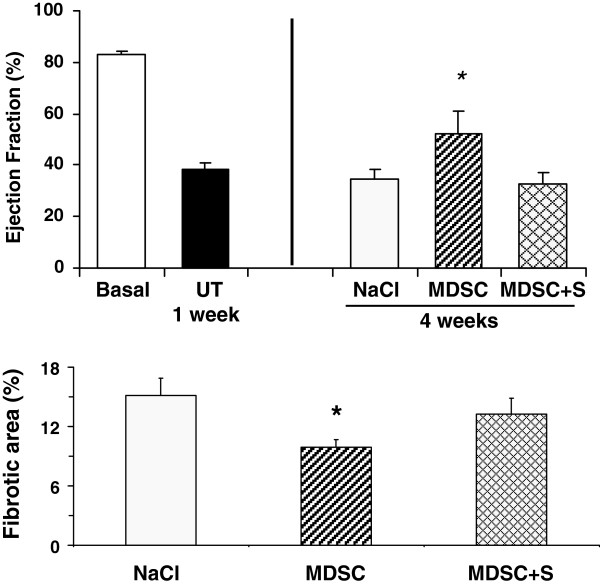
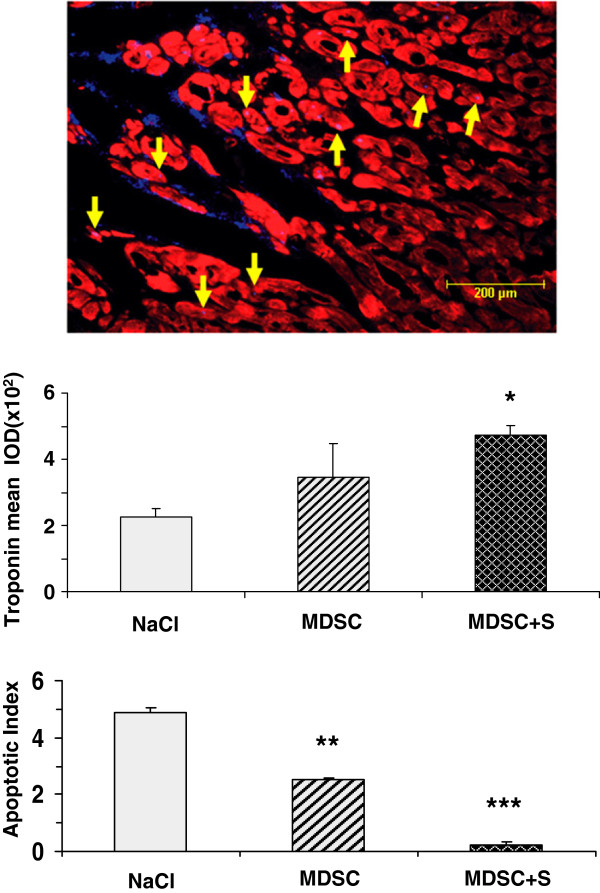
Results: As compared to untreated MI rats, sildenafil improved LVEF, reduced collagen, myofibroblasts, and circulating MMPs, and increased cardiac troponin T. MDSC replicated most of these effects and stimulated cardiac angiogenesis. Concurrent MDSC/sildenafil counteracted cardiomyocyte and endothelial cells loss, but did not improve LVEF or angiogenesis, and upregulated PDE 5.
Conclusions: Long-term oral sildenafil, or MDSC given separately, reduce the MI fibrotic scar and improve left ventricular function in this rat model. The failure of the treatment combination may be due to inducing overexpression of PDE5.
Figures
Similar articles
-
Separate or combined treatments with daily sildenafil, molsidomine, or muscle-derived stem cells prevent erectile dysfunction in a rat model of cavernosal nerve damage.J Sex Med. 2012 Nov;9(11):2814-26. doi: 10.1111/j.1743-6109.2012.02913.x. Epub 2012 Sep 13. J Sex Med. 2012. PMID: 22974131 Free PMC article.
-
L-arginine and phosphodiesterase (PDE) inhibitors counteract fibrosis in the Peyronie's fibrotic plaque and related fibroblast cultures.Nitric Oxide. 2003 Dec;9(4):229-44. doi: 10.1016/j.niox.2003.12.002. Nitric Oxide. 2003. PMID: 14996430
-
Phosphodiesterase 5A inhibition induces Na+/H+ exchanger blockade and protection against myocardial infarction.Hypertension. 2007 May;49(5):1095-103. doi: 10.1161/HYPERTENSIONAHA.107.087759. Epub 2007 Mar 5. Hypertension. 2007. PMID: 17339532
-
Phosphodiesterase type 5 inhibitors in pulmonary arterial hypertension.Adv Ther. 2009 Sep;26(9):813-25. doi: 10.1007/s12325-009-0064-z. Epub 2009 Sep 19. Adv Ther. 2009. PMID: 19768639 Review.
-
Up and down-regulation of phosphodiesterase-5 as related to tachyphylaxis and priapism.J Urol. 2003 Aug;170(2 Pt 2):S15-8; discussion S19. doi: 10.1097/01.ju.0000075500.11519.e8. J Urol. 2003. PMID: 12853767 Review.
Cited by
-
Myostatin genetic inactivation inhibits myogenesis by muscle-derived stem cells in vitro but not when implanted in the mdx mouse muscle.Stem Cell Res Ther. 2013 Jan 7;4(1):4. doi: 10.1186/scrt152. Stem Cell Res Ther. 2013. PMID: 23295128 Free PMC article.
-
Microenergy acoustic pulses induced myogenesis of urethral striated muscle stem/progenitor cells.Transl Androl Urol. 2019 Oct;8(5):489-500. doi: 10.21037/tau.2019.08.18. Transl Androl Urol. 2019. PMID: 32133280 Free PMC article.
-
Dyslipidemia Is a Major Factor in Stem Cell Damage Induced by Uncontrolled Long-Term Type 2 Diabetes and Obesity in the Rat, as Suggested by the Effects on Stem Cell Culture.J Sex Med. 2018 Dec;15(12):1678-1697. doi: 10.1016/j.jsxm.2018.09.019. J Sex Med. 2018. PMID: 30527052 Free PMC article.
-
Regulation and Pharmacology of the Cyclic GMP and Nitric Oxide Pathway in Embryonic and Adult Stem Cells.Cells. 2024 Dec 5;13(23):2008. doi: 10.3390/cells13232008. Cells. 2024. PMID: 39682756 Free PMC article. Review.
-
Implanted Muscle-Derived Stem Cells Ameliorate Erectile Dysfunction in a Rat Model of Type 2 Diabetes, but Their Repair Capacity Is Impaired by Their Prior Exposure to the Diabetic Milieu.J Sex Med. 2016 May;13(5):786-97. doi: 10.1016/j.jsxm.2016.02.168. J Sex Med. 2016. PMID: 27114192 Free PMC article.
References
-
- Kovanecz I, Nolazco G, Ferrini MG, Toblli JE, Heydarkhan S, Vernet D, Rajfer J, Gonzalez-Cadavid NF. Early onset of fibrosis within the arterial media in a rat model of type 2 diabetes mellitus with erectile dysfunction. BJU Int. 2009;103:1396–1404. doi: 10.1111/j.1464-410X.2008.08251.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
