

Cardiotoxicity in childhood cancer survivors: strategies for prevention and management
- PMID: 22871201
- PMCID: PMC3870660
- DOI: 10.2217/fca.12.44
Cardiotoxicity in childhood cancer survivors: strategies for prevention and management
Abstract
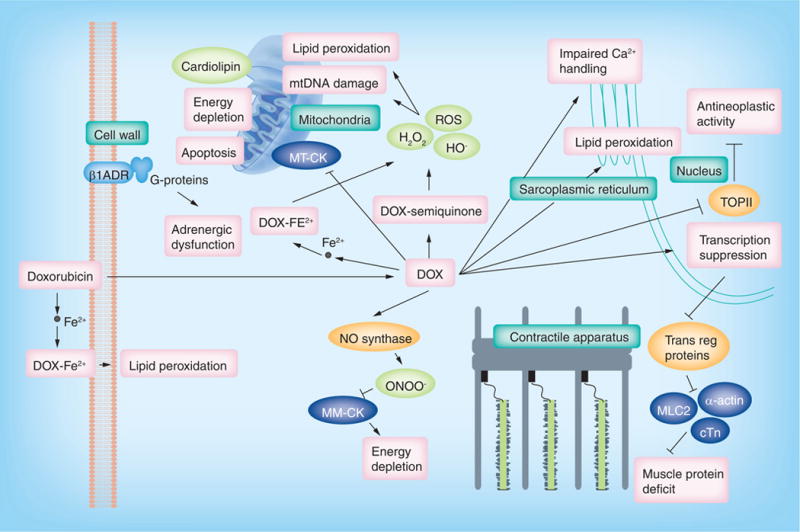
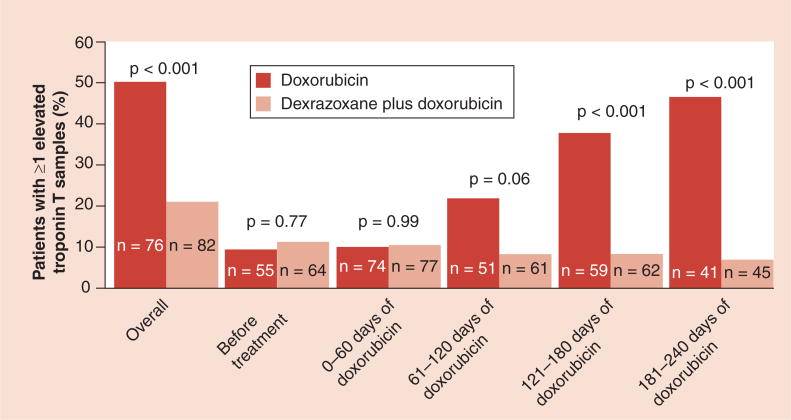
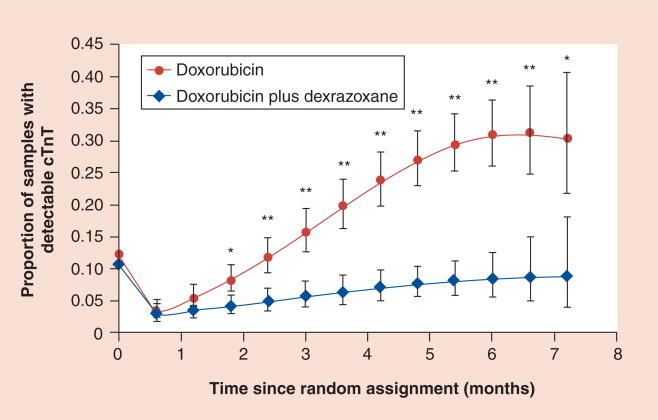
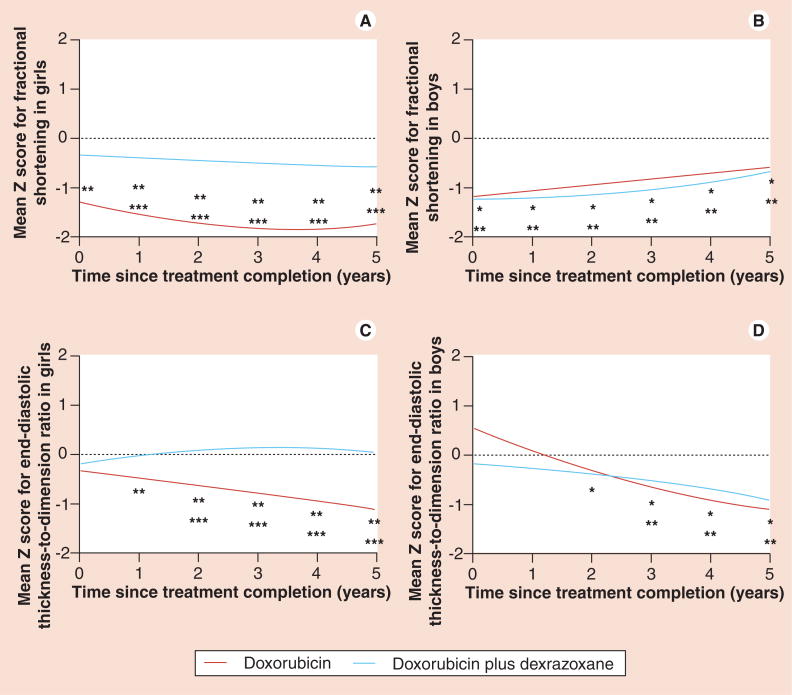
Advances in cancer treatment have greatly improved survival rates of children with cancer. However, these same chemotherapeutic or radiologic treatments may result in long-term health consequences. Anthracyclines, chemotherapeutic drugs commonly used to treat children with cancer, are known to be cardiotoxic, but the mechanism by which they induce cardiac damage is still not fully understood. A higher cumulative anthracycline dose and a younger age of diagnosis are only a few of the many risk factors that identify the children at increased risk of developing cardiotoxicity. While cardiotoxicity can develop at anytime, starting from treatment initiation and well into adulthood, identifying the best cardioprotective measures to minimize the long-term damage caused by anthracyclines in children is imperative. Dexrazoxane is the only known agent to date, that is associated with less cardiac dysfunction, without reducing the oncologic efficacy of the anthracycline doxorubicin in children. Given the serious long-term health consequences of cancer treatments on survivors of childhood cancers, it is essential to investigate new approaches to improving the safety of cancer treatments.
Figures
References
-
- Mariotto AB, Rowland JH, Yabroff KR, et al. Long-term survivors of childhood cancers in the United States. Cancer Epidemiol Biomarkers Prev. 2009;18:1033–1040. - PubMed
-
- Hinkle AS, Proukou C, French CA, et al. A clinic-based, comprehensive care model for studying late effects in long-term survivors of pediatric illnesses. Pediatrics. 2004;113(Suppl 4):1141–1145. - PubMed
-
- Reulen RC, Winter DL, Frobisher C, et al. Long-term cause-specific mortality among survivors of childhood cancer. JAMA. 2010;304(2):172–179. - PubMed
-
- van der Pal HJ, van Dalen EC, van Delden E, et al. High risk of symptomatic cardiac events in childhood cancer survivors. J Clin Oncol. 2012;30(13):1429–1437. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical