

Association of weight status with mortality in adults with incident diabetes
- PMID: 22871870
- PMCID: PMC3467944
- DOI: 10.1001/jama.2012.9282
Association of weight status with mortality in adults with incident diabetes
Erratum in
- JAMA. 2012 Nov 28;308(20):2085
Abstract
Context: Type 2 diabetes in normal-weight adults (body mass index [BMI] <25) is a representation of the metabolically obese normal-weight phenotype with unknown mortality consequences.
Objective: To test the association of weight status with mortality in adults with new-onset diabetes in order to minimize the influence of diabetes duration and voluntary weight loss on mortality.
Design, setting, and participants: Pooled analysis of 5 longitudinal cohort studies: Atherosclerosis Risk in Communities study, 1990-2006; Cardiovascular Health Study, 1992-2008; Coronary Artery Risk Development in Young Adults, 1987-2011; Framingham Offspring Study, 1979-2007; and Multi-Ethnic Study of Atherosclerosis, 2002-2011. A total of 2625 participants with incident diabetes contributed 27,125 person-years of follow-up. Included were men and women (age >40 years) who developed incident diabetes based on fasting glucose 126 mg/dL or greater or newly initiated diabetes medication and who had concurrent measurements of BMI. Participants were classified as normal weight if their BMI was 18.5 to 24.99 or overweight/obese if BMI was 25 or greater.
Main outcome measures: Total, cardiovascular, and noncardiovascular mortality.
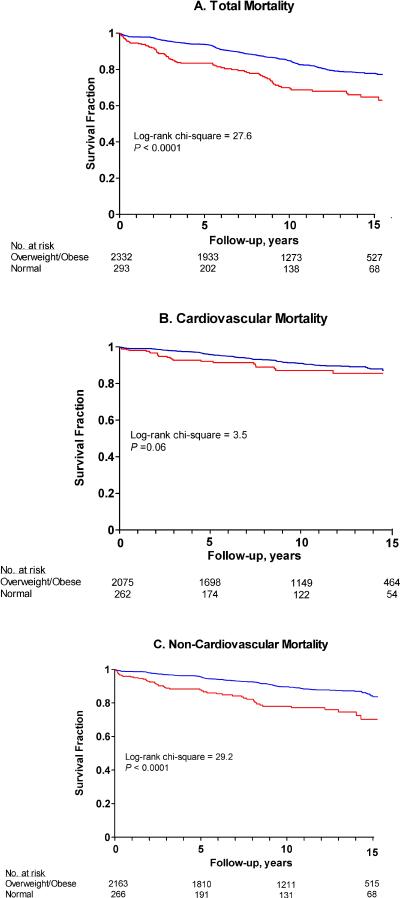
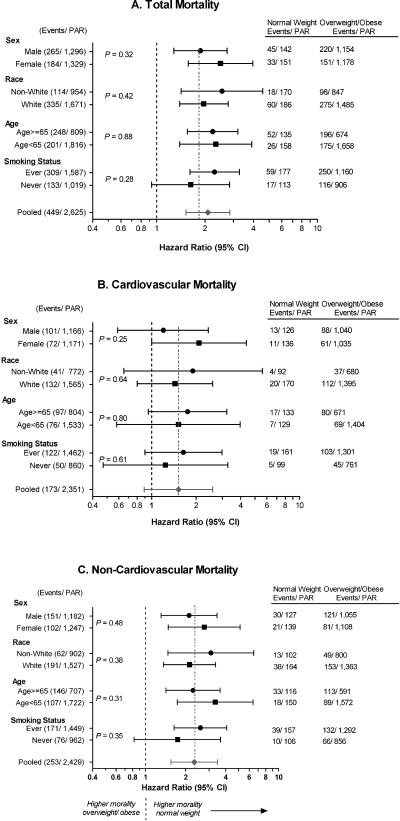
Results: The proportion of adults who were normal weight at the time of incident diabetes ranged from 9% to 21% (overall 12%). During follow-up, 449 participants died: 178 from cardiovascular causes and 253 from noncardiovascular causes (18 were not classified). The rates of total, cardiovascular, and noncardiovascular mortality were higher in normal-weight participants (284.8, 99.8, and 198.1 per 10,000 person-years, respectively) than in overweight/obese participants (152.1, 67.8, and 87.9 per 10,000 person-years, respectively). After adjustment for demographic characteristics and blood pressure, lipid levels, waist circumference, and smoking status, hazard ratios comparing normal-weight participants with overweight/obese participants for total, cardiovascular, and noncardiovascular mortality were 2.08 (95% CI, 1.52-2.85), 1.52 (95% CI, 0.89-2.58), and 2.32 (95% CI, 1.55-3.48), respectively.
Conclusion: Adults who were normal weight at the time of incident diabetes had higher mortality than adults who are overweight or obese.
Figures
Comment in
-
Beyond the obesity paradox in diabetes: fitness, fatness, and mortality.JAMA. 2012 Aug 8;308(6):619-20. doi: 10.1001/jama.2012.9776. JAMA. 2012. PMID: 22871873 No abstract available.
-
Diabetes: Weight status affects mortality risk.Nat Rev Endocrinol. 2012 Oct;8(10):567. doi: 10.1038/nrendo.2012.152. Epub 2012 Aug 28. Nat Rev Endocrinol. 2012. PMID: 22926099 No abstract available.
-
[Type 2 diabete: Do patients with normal weight die earlier? - Higher mortality is not restricted to overweight patients].Dtsch Med Wochenschr. 2012 Oct;137(42):2140. doi: 10.1055/s-0032-1329025. Epub 2012 Oct 10. Dtsch Med Wochenschr. 2012. PMID: 23055352 German. No abstract available.
-
Weight and mortality in adults with diabetes.JAMA. 2012 Nov 28;308(20):2079; author reply 2080-1. doi: 10.1001/jama.2012.14567. JAMA. 2012. PMID: 23188014 No abstract available.
-
Weight and mortality in adults with diabetes.JAMA. 2012 Nov 28;308(20):2079-80; author reply 2080-1. doi: 10.1001/jama.2012.14564. JAMA. 2012. PMID: 23188015 No abstract available.
-
Weight and mortality in adults with diabetes.JAMA. 2012 Nov 28;308(20):2080; author reply 2080-1. doi: 10.1001/jama.2012.14561. JAMA. 2012. PMID: 23188016 No abstract available.
References
-
- Ruderman NB, Schneider SH, Berchtold P. The “metabolically-obese,” normal-weight individual. Am J Clin Nutr. 1981;34(8):1617–1621. - PubMed
-
- Gregg EW, Cadwell BL, Cheng YJ, et al. Trends in the prevalence and ratio of diagnosed to undiagnosed diabetes according to obesity levels in the U.S. Diabetes Care. 2004;27(12):2806–2812. - PubMed
-
- Uretsky S, Messerli FH, Bangalore S, et al. Obesity paradox in patients with hypertension and coronary artery disease. Am J Med. 2007;120(10):863–870. - PubMed
-
- Schmidt D, Salahudeen A. The Obesity-Survival Paradox in Hemodialysis Patients: Why Do Overweight Hemodialysis Patients Live Longer? Nutrition in Clinical Practice. 2007;22(1):11–15. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- R56 AG020098/AG/NIA NIH HHS/United States
- N01-HC-48049/HC/NHLBI NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- N01 HC048050/HL/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- N01 HC095095/HL/NHLBI NIH HHS/United States
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- N01 HC048048/HL/NHLBI NIH HHS/United States
- N01 HC055019/HL/NHLBI NIH HHS/United States
- R01 HL078972/HL/NHLBI NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01-HC-48047/HC/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- P30 DK079637/DK/NIDDK NIH HHS/United States
- N01 HC048049/HL/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC055015/HL/NHLBI NIH HHS/United States
- AG-20098/AG/NIA NIH HHS/United States
- N01-HC-95095/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01-HC-48050/HC/NHLBI NIH HHS/United States
- AG-027058/AG/NIA NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01 HC-55222/HC/NHLBI NIH HHS/United States
- R21 DK082903/DK/NIDDK NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- 5 R01 HL078972/HL/NHLBI NIH HHS/United States
- N01 HC048047/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- N01-HC-85239/HC/NHLBI NIH HHS/United States
- N01-HC-48048/HC/NHLBI NIH HHS/United States
- AG-023629/AG/NIA NIH HHS/United States
- N01 HC075150/HL/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- R01 AG027058/AG/NIA NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC045133/HC/NHLBI NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
- R21DK082903/DK/NIDDK NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
