

Effect of tight glucose control with insulin on the thyroid axis of critically ill children and its relation with outcome
- PMID: 22872689
- PMCID: PMC3462949
- DOI: 10.1210/jc.2012-2240
Effect of tight glucose control with insulin on the thyroid axis of critically ill children and its relation with outcome
Abstract
Context: Tight glucose control (TGC) to normal-for-age fasting blood glucose levels reduced morbidity and mortality in surgical adult and pediatric intensive care unit (ICU) patients. In adults, TGC did not affect the illness-induced alterations in thyroid hormones. With better feeding in children than in adult patients, we hypothesized that TGC in pediatric ICU patients reactivates the thyroid axis.
Objective: The aim of this study was to assess the impact of TGC on the thyroid axis in pediatric ICU patients and to investigate how these changes affect the TGC outcome benefit.
Design and patients: We conducted a preplanned analysis of all patients not treated with thyroid hormone, dopamine, or corticosteroids who were included in a randomized controlled trial on TGC (n=700).
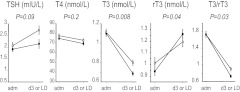
Main outcome measures: Serum TSH, T4, T3, and rT3 were measured upon admission and on ICU day 3 or the last ICU day for patients discharged earlier. Changes from baseline were compared for the TGC and usual care groups. The impact on the outcome benefit of TGC was assessed with multivariable Cox proportional hazard analysis, correcting for baseline risk factors.
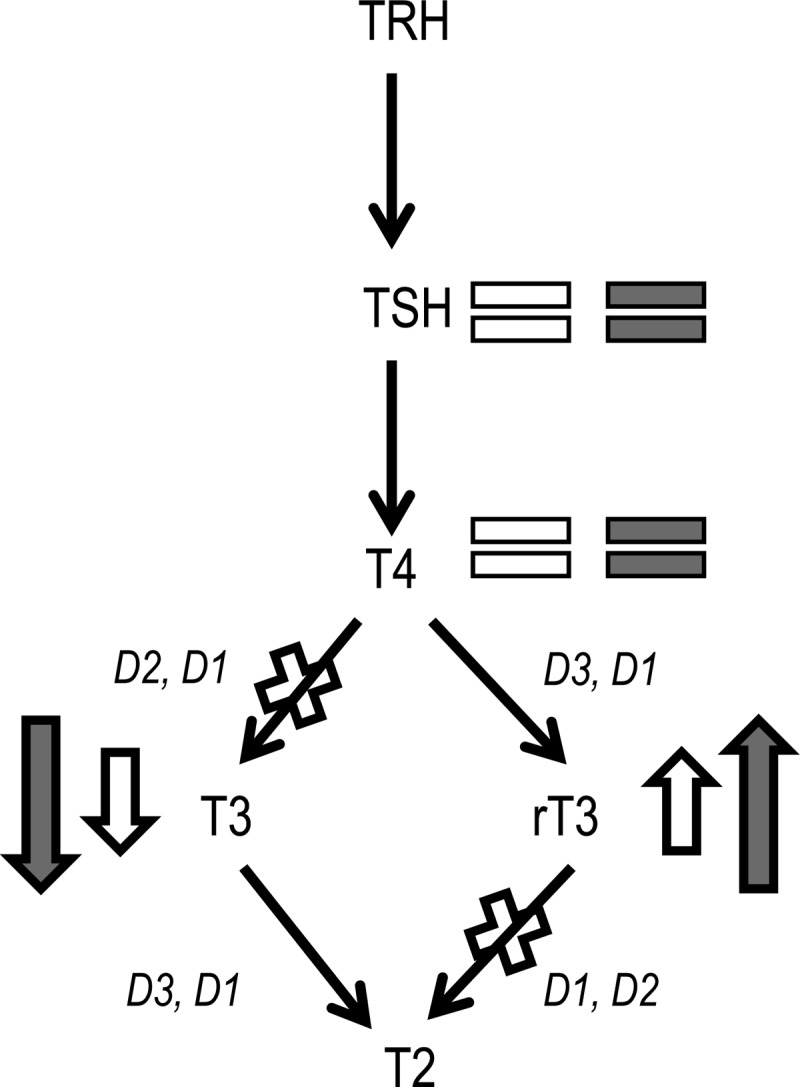
Results: TGC further lowered the T)/rT3 ratio (P=0.03), whereas TSH (P=0.09) and T4 (P=0.3) were unaltered. With TGC, the likelihood of earlier live discharge from the ICU was 19% higher at any time (hazard ratio, 1.190; 95% confidence interval, 1.010-1.407; P=0.03). This benefit was statistically explained by the further reduction of T3/rT3 with TGC because an increase in T3/rT3 was strongly associated with a lower likelihood for earlier live discharge (hazard ratio per unit increase, 0.863; 95% confidence interval, 0.806-0.927; P<0.0001).
Conclusions: TGC further accentuated the peripheral inactivation of thyroid hormone. This effect, mimicking a fasting response, statistically explained part of the clinical outcome benefit of TGC.
Trial registration: ClinicalTrials.gov NCT00214916.
Figures
References
-
- Gardner DF, Kaplan MM, Stanley CA, Utiger RD. 1979. Effect of tri-iodothyronine replacement on the metabolic and pituitary responses to starvation. N Engl J Med 300:579–584 - PubMed
-
- Hugues JN, Burger AG, Pekary AE, Hershman JM. 1984. Rapid adaptations of serum thyrotrophin, triiodothyronine and reverse triiodothyronine levels to short-term starvation and refeeding. Acta Endocrinol (Copenh) 105:194–199 - PubMed
-
- Van den Berghe G, de Zegher F, Bouillon R. 1998. Clinical review 95: acute and prolonged critical illness as different neuroendocrine paradigms. J Clin Endocrinol Metab 83:1827–1834 - PubMed
-
- van der Poll T, Romijn JA, Wiersinga WM, Sauerwein HP. 1990. Tumor necrosis factor: a putative mediator of the sick euthyroid syndrome in man. J Clin Endocrinol Metab 71:1567–1572 - PubMed
-
- Peeters RP, Wouters PJ, Kaptein E, van Toor H, Visser TJ, Van den Berghe G. 2003. Reduced activation and increased inactivation of thyroid hormone in tissues of critically ill patients. J Clin Endocrinol Metab 88:3202–3211 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
