

Covert checks by standardised patients of general practitioners' delivery of new periodic health examinations: clustered cross-sectional study from a consumer organisation
- PMID: 22872721
- PMCID: PMC4400678
- DOI: 10.1136/bmjopen-2011-000744
Covert checks by standardised patients of general practitioners' delivery of new periodic health examinations: clustered cross-sectional study from a consumer organisation
Abstract
Objective: To assess if data collected by a consumer organisation are valid for a health service research study on physicians' performance in preventive care. To report first results of the analysis of physicians performance like consultation time and guideline adherence in history taking.
Design: Secondary data analysis of a clustered cross-sectional direct observation survey.
Setting: General practitioners (GPs) in Vienna, Austria, visited unannounced by mystery shoppers (incognito standardised patients (ISPs)).
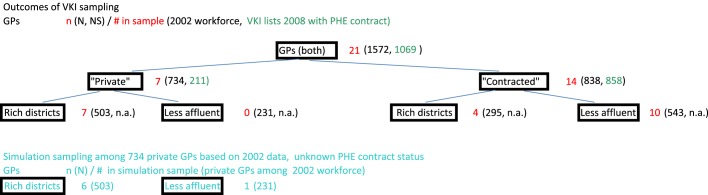
Participants: 21 randomly selected GPs were visited by two different ISPs each. 40 observation protocols were realised.
Main outcome measures: Robustness of sampling and data collection by the consumer organisation. GPs consultation and waiting times, guideline adherence in history taking.
Results: The double stratified random sampling method was robust and representative for the private and contracted GPs mix of Vienna. The clinical scenarios presented by the ISPs were valid and believable, and no GP realised the ISPs were not genuine patients. The average consultation time was 46 min (95% CI 37 to 54 min). Waiting times differed more than consultation times between private and contracted GPs. No differences between private and contracted GPs in terms of adherence to the evidence-based guidelines regarding history taking including questions regarding alcohol use were found. According to the analysis, 20% of the GPs took a perfect history (95% CI 9% to 39%).
Conclusions: The analysis of secondary data collected by a consumer organisation was a valid method for drawing conclusions about GPs preventive practice. Initial results, like consultation times longer than anticipated, and the moderate quality of history taking encourage continuing the analysis on available clinical data.
Conflict of interest statement
Figures

References
-
- Baker R, Camosso SJ, Gillies C, et al. Tailored interventions to overcome identified barriers to change: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2010;(3):CD005470. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005470 - DOI - PMC - PubMed
-
- Fletcher SW, Spitzer WO. Approach of the Canadian Task Force to the Periodic Health Examination. Ann Intern Med 1980;92:253–4. - PubMed
-
- Hudon E, Beaulieu MD, Roberge D. Integration of the recommendations of the Canadian Task Force on Preventive Health Care: obstacles perceived by a group of family physicians. Fam Pract 2004;21:11–17. - PubMed
LinkOut - more resources
Full Text Sources