

Pharmacists' recommendations to improve care transitions
- PMID: 22872752
- PMCID: PMC3575733
- DOI: 10.1345/aph.1Q641
Pharmacists' recommendations to improve care transitions
Abstract
Background: Increasingly, hospitals are implementing multifaceted programs to improve medication reconciliation and transitions of care, often involving pharmacists.
Objective: To assess pharmacists' views on their roles in hospital-based medication reconciliation and discharge counseling and provide their recommendations for improving care transitions.
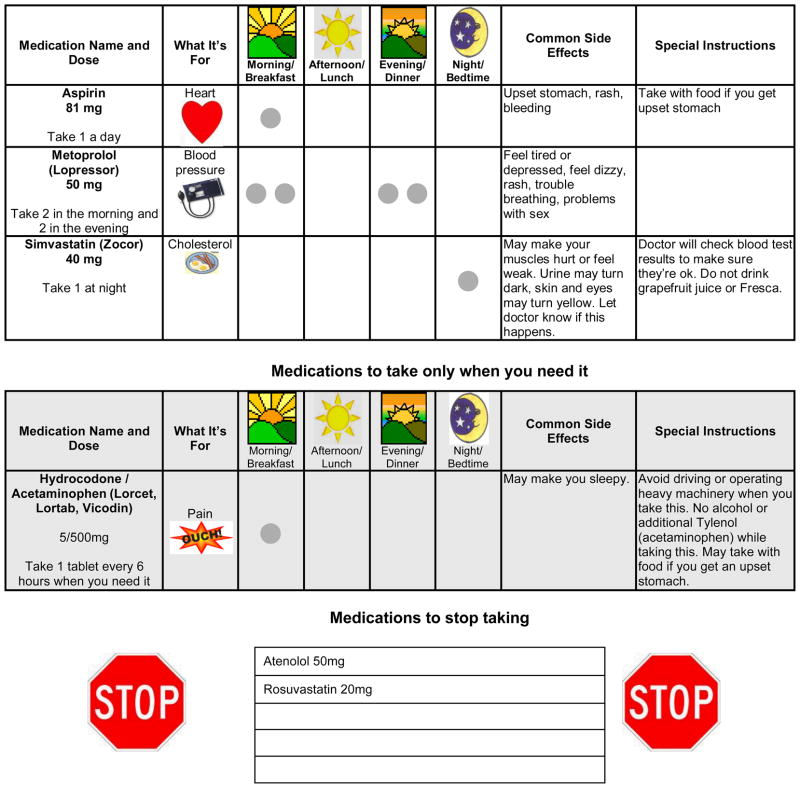
Methods: Eleven study pharmacists at 2 hospitals participated in the Pharmacist Intervention for Low Literacy in Cardiovascular Disease (PILL-CVD) study and completed semistructured one-on-one interviews, which were coded systematically in NVivo. Pharmacists provided their perspectives on admission and discharge medication reconciliation, in-hospital patient counseling, provision of simple medication adherence aids (eg, pill box, illustrated daily medication schedule), and telephone follow-up.
Results: Pharmacists indicated that they considered medication reconciliation, although time consuming, to be their most important role in improving care transitions, particularly through detection of errors that required correction in the admission medication history. They also identified patients who required additional counseling because of poor understanding of their medications. Providing adherence aids was felt to be highly valuable for patients with low health literacy, although less useful for patients with adequate health literacy. Pharmacists noted that having trained administrative staff conduct initial postdischarge follow-up calls to screen for issues and triage which patients needed pharmacist follow-up was helpful and an efficient use of resources. Pharmacists' recommendations for improving care transitions included clear communication among team members, protected time for discharge counseling, patient and family engagement in discharge counseling, and provision of patient education materials.
Conclusions: Pharmacists are well positioned to participate in hospital-based medication reconciliation, identify patients with poor medication understanding or adherence, and provide tailored patient counseling to improve transitions of care. Additional studies are needed to confirm these findings in other settings and to determine the efficacy and cost-effectiveness of different models of pharmacist involvement.
Conflict of interest statement
Katherine Taylor Haynes has no potential conflicts of interest to disclose.
Alison Oberne has no potential conflicts of interest to disclose.
Courtney Cawthon has no potential conflicts of interest to disclose.
Potential conflict of interest: Dr. Kripalani is a consultant to and holds equity in PictureRx, LLC. The terms of this agreement were reviewed and approved by Vanderbilt University in accordance with its conflict of interest policies. PictureRx provided no materials or funding for this study.
Figures
Similar articles
-
Evaluation of Pharmacist-Initiated Discharge Medication Reconciliation and Patient Counseling Procedures.Consult Pharm. 2018 Apr 1;33(4):222-226. doi: 10.4140/TCP.n.2018.222. Consult Pharm. 2018. PMID: 29609701
-
Inpatient pharmacists' patient referrals to a transitions-of-care pharmacist: Evaluation of an automated referral process.J Am Pharm Assoc (2003). 2018 Sep-Oct;58(5):540-546. doi: 10.1016/j.japh.2018.05.007. Epub 2018 Jul 17. J Am Pharm Assoc (2003). 2018. PMID: 30017369
-
Variations in pharmacy-based transition-of-care activities in the United States: a national survey.Am J Health Syst Pharm. 2014 Apr 15;71(8):648-56. doi: 10.2146/ajhp130510. Am J Health Syst Pharm. 2014. PMID: 24688039
-
Pharmacist-led medication reconciliation at patient discharge: A scoping review.Res Social Adm Pharm. 2020 May;16(5):605-613. doi: 10.1016/j.sapharm.2019.08.001. Epub 2019 Aug 1. Res Social Adm Pharm. 2020. PMID: 31395445
-
Preventing medication errors in transitions of care: A patient case approach.J Am Pharm Assoc (2003). 2015 Mar-Apr;55(2):e264-74; quiz e275-6. doi: 10.1331/JAPhA.2015.15509. J Am Pharm Assoc (2003). 2015. PMID: 25749270 Review.
Cited by
-
Impact of medication reconciliation and review and counselling, on adverse drug events and healthcare resource use.Int J Clin Pharm. 2018 Oct;40(5):1154-1164. doi: 10.1007/s11096-018-0650-8. Epub 2018 May 12. Int J Clin Pharm. 2018. PMID: 29754251 Clinical Trial.
-
Characteristics associated with postdischarge medication errors.Mayo Clin Proc. 2014 Aug;89(8):1042-51. doi: 10.1016/j.mayocp.2014.04.023. Epub 2014 Jul 3. Mayo Clin Proc. 2014. PMID: 24998906 Free PMC article.
-
Medication literacy status of outpatients in ambulatory care settings in Changsha, China.J Int Med Res. 2017 Feb;45(1):303-309. doi: 10.1177/0300060516676726. Epub 2017 Jan 12. J Int Med Res. 2017. PMID: 28222647 Free PMC article.
-
Pharmacy-Initiated Transitions of Care Services: An Opportunity to Impact Patient Satisfaction.Hosp Pharm. 2015 Nov;50(10):911-917. doi: 10.1310/hpj5010-911. Epub 2015 Nov 19. Hosp Pharm. 2015. PMID: 27729679 Free PMC article.
-
Improving pediatric liquid medication labeling of the hospital information system in Malaysia: qualitative analysis of pharmacists' perceptions.Pharm Pract (Granada). 2016 Apr-Jun;14(2):699. doi: 10.18549/PharmPract.2016.02.699. Epub 2016 Jun 15. Pharm Pract (Granada). 2016. PMID: 27382422 Free PMC article.
References
-
- DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008:1–20. - PubMed
-
- Kripalani S, Jackson AT, Schnipper JL, Coleman EA. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2:314–323. - PubMed
-
- Kripalani S, Henderson LE, Jacobson TA, Vaccarino V. Medication use among inner-city patients after hospital discharge: patient reported barriers and solutions. Mayo Clin Proc. 2008;83:529–535. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
