

Recurrent Mastitis after Core Needle Biopsy: Case Report of an Unusual Complication after Core Needle Biopsy of a Phyllodes Tumor
- PMID: 22872800
- PMCID: PMC3409383
- DOI: 10.1159/000339689
Recurrent Mastitis after Core Needle Biopsy: Case Report of an Unusual Complication after Core Needle Biopsy of a Phyllodes Tumor
Abstract
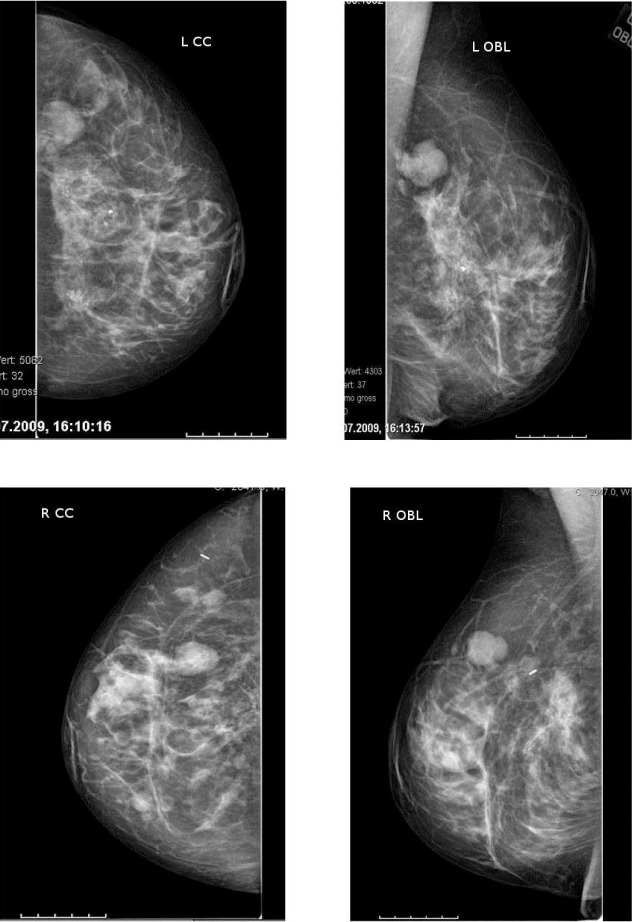
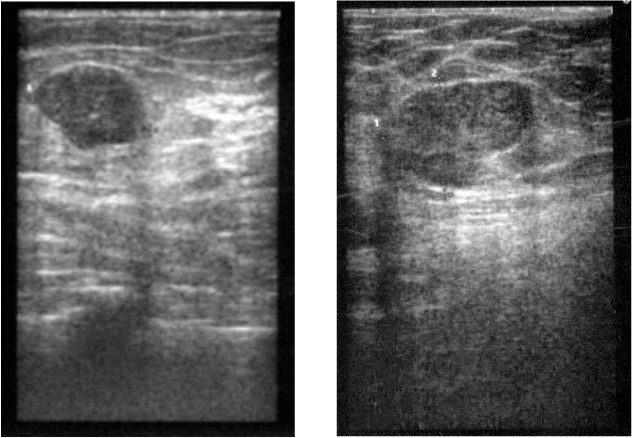
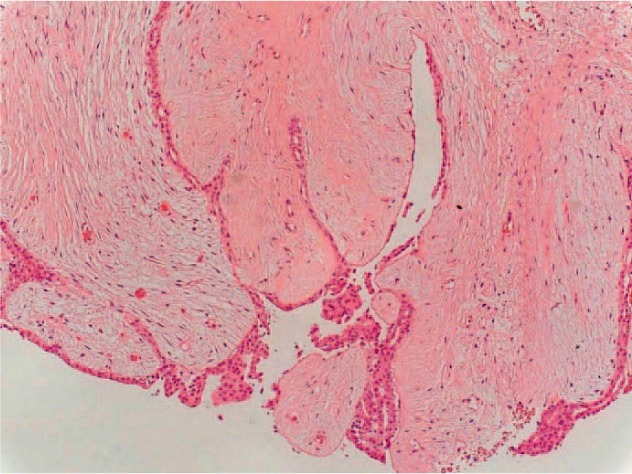
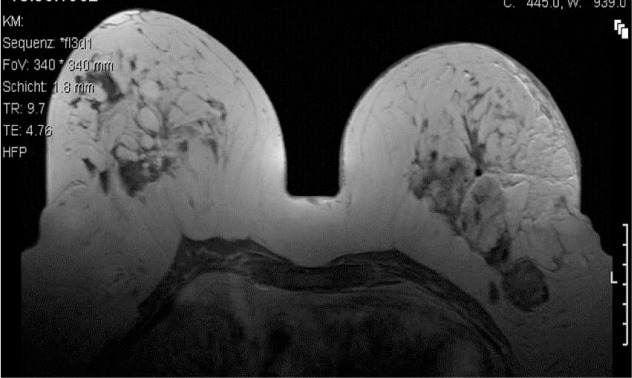
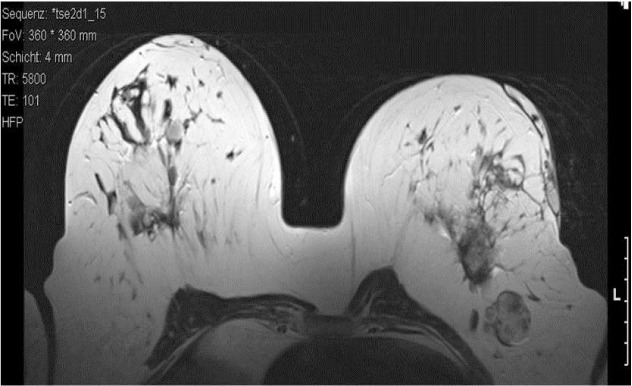
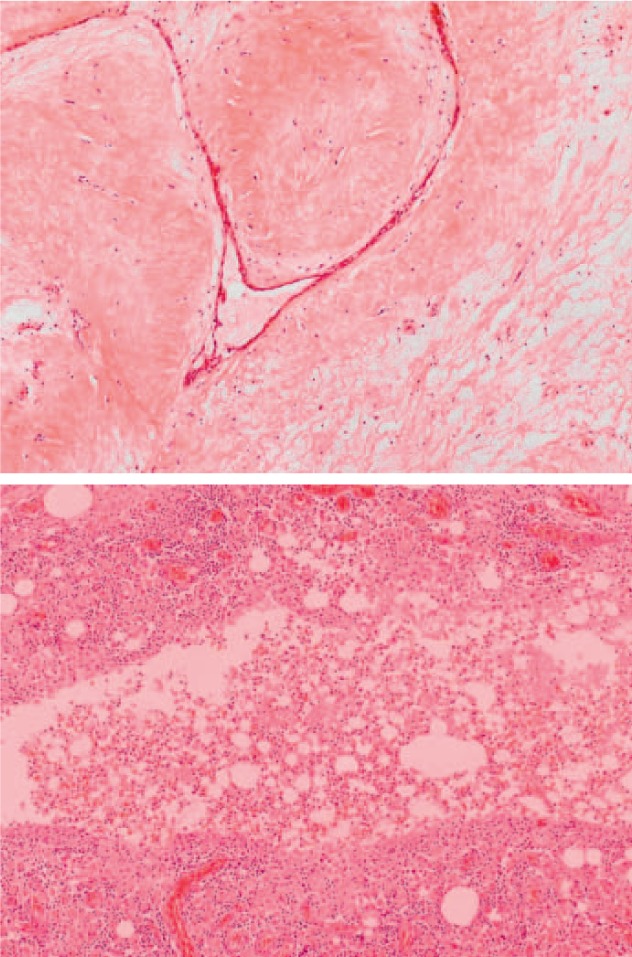
BACKGROUND: In the routine work-up of suspect breast lesions, ultrasound-controlled core needle biopsy (CNB) is the most common tool to acquire tissue for histopathologic analysis in a safe, quick and convenient way. Complications are generally rare. The most common complications are hematoma and infection, each with less than 1 in 1000 cases. CASE REPORT: Here, we present a case of a 48-year-old patient who underwent CNB for several lesions that were assessed as Breast Imaging Report and Data System (BI-RADS) IV in breast ultrasound and mammography. In the past, she had had 2 bilateral breast reduction surgeries and 1 open biopsy of a fibroadenoma. Histology revealed a phyllodes tumor. Following this, mastitis occurred which was resistant to common conservative measurements such as intravenous antibiotics over months. Finally, mastectomy was performed, followed by adequate wound healing. CONCLUSIONS: In the presented case, the prolonged course of breast infection after CNB was not as expected. If this occurs, conservative treatment with antibiotics can be initiated. Possible additional risk factors such as diabetes mellitus, steroid therapy, or immunosuppression should be identified. However, in case of missing recovery, wide surgical excision is recommended.
Hintergrund: Zur Abklärung von auffälligen sonographischen Befunden in der Brust gehört in der Hauptsache die Stanzbiopsie. Sie stellt eine bequeme, schnelle und komplikationsarme Methode zur Asservierung von Gewebe zur histopathologischen Diagnosesicherung dar. In sehr seltenen Fällen (weniger als 1/1000) treten Nebenwirkungen wie Hämatome oder Infektionen auf, die in aller Regel gut behandelbar sind.
Fallbericht: Wir möchten hier den Fall einer 48-jährigen Patientin schildern, die aufgrund eines Breast Imaging Report and Data System (BI-RADS) IV-begutach-teten mammasonographischen Befundes eine Stanzbiopsie erhalten hat. In der Vergangenheit wurden bei der Patientin bereits 2 Operationen zur Brustreduktion sowie 1 offene Probeexzision bei einem Fibroadenom durchgeführt. Nach der Biopsie entwickelte die Patientin eine therapierefraktäre Mastitis, die über Monate trotz intensiver konservativer Maßnahmen wie intravenöse Antibiose nicht beherrschbar war. In der Konsequenz wurde eine Mastektomie durchgeführt, an die sich eine adäquate Wundheilung anschloss.
Schlussfolgerungen: Auch wenn es eine täglich eingesetzte, komplikationsarme Methode ist, sollte bei der Anwendung einer Stanzbiopsie an Komplikationen wie Hämatom oder Infektion gedacht werden, gerade wenn Risikofaktoren wie Diabetes mellitus, Kortikoidtherapie oder Immunsuppression hinzukommen. Bei ausbleibender Besserung ist die operative Sanierung zu empfehlen.
Figures

Similar articles
-
Clinical and radiologic data and core needle biopsy findings should dictate management of cellular fibroepithelial tumors of the breast.Breast J. 2010 Nov-Dec;16(6):573-80. doi: 10.1111/j.1524-4741.2010.01013.x. Breast J. 2010. PMID: 21070433
-
Clinical practice guidelines from the French College of Gynecologists and Obstetricians (CNGOF): benign breast tumors - short text.Eur J Obstet Gynecol Reprod Biol. 2016 May;200:16-23. doi: 10.1016/j.ejogrb.2016.02.017. Epub 2016 Feb 28. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 26967341
-
Differential diagnosis between fibroadenoma, giant fibroadenoma and phyllodes tumour: sonographic features and core needle biopsy.Radiol Med. 2011 Sep;116(6):905-18. doi: 10.1007/s11547-011-0672-y. Epub 2011 Apr 19. Radiol Med. 2011. PMID: 21509559 English, Italian.
-
Core needle biopsy diagnosis of fibroepithelial lesions of the breast: a diagnostic challenge.Pathology. 2020 Oct;52(6):627-634. doi: 10.1016/j.pathol.2020.06.005. Epub 2020 Aug 6. Pathology. 2020. PMID: 32771211 Review.
-
Clinical management issues in percutaneous core breast biopsy.Radiol Clin North Am. 2000 Jul;38(4):791-807. doi: 10.1016/s0033-8389(05)70201-3. Radiol Clin North Am. 2000. PMID: 10943278 Review.
Cited by
-
Breast Lesions during Pregnancy - a Diagnostic Challenge: Case Report.Breast Care (Basel). 2015 Jul;10(3):207-10. doi: 10.1159/000381823. Epub 2015 Apr 28. Breast Care (Basel). 2015. PMID: 26557826 Free PMC article.
References
-
- Bruening W, Fontanarosa J, Tipton K, Treadwell JR, Launders J, Schoelles K. Systematic review: comparative effectiveness of core-needle and open surgical biopsy to diagnose breast lesions. Ann Intern Med. 2010;152:238–246. - PubMed
-
- Lindgren PG. Percutaneous needle biopsy. A new technique. Acta Radiol Diagn (Stockh) 1982;23:653–656. - PubMed
-
- Parker SH, Jobe WE, Dennis MA, Stavros AT, Johnson KK, Yakes WF, Truell JE, Price JG, Kortz AB, Clark DG. US-guided automated large-core breast biopsy. Radiology. 1993;187:507–511. - PubMed
-
- Liberman L. Centennial dissertation. Percutaneous imaging-guided core breast biopsy: state of the art at the millennium. AJR Am J Roentgenol. 2000;174:1191–1199. - PubMed
-
- Parker SH, Burbank F, Jackman RJ, Aucreman CJ, Cardenosa G, Cink TM, Coscia JL, Jr, Eklund GW, Evans WP, III, Garver PR. Percutaneous large-core breast biopsy: a multi-institutional study. Radiology. 1994;193:359–364. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
