

Fluid management in critically ill patients: the role of extravascular lung water, abdominal hypertension, capillary leak, and fluid balance
- PMID: 22873410
- PMCID: PMC3390304
- DOI: 10.1186/2110-5820-2-S1-S1
Fluid management in critically ill patients: the role of extravascular lung water, abdominal hypertension, capillary leak, and fluid balance
Abstract
Introduction: Capillary leak in critically ill patients leads to interstitial edema. Fluid overload is independently associated with poor prognosis. Bedside measurement of intra-abdominal pressure (IAP), extravascular lung water index (EVLWI), fluid balance, and capillary leak index (CLI) may provide a valuable prognostic tool in mechanically ventilated patients.
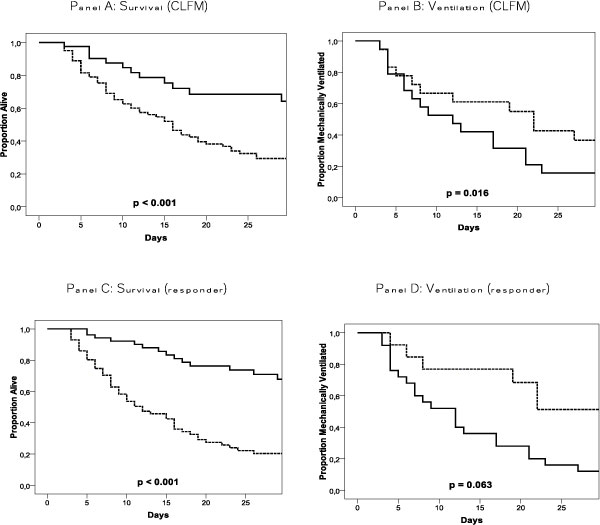
Methods: We performed an observational study of 123 mechanically ventilated patients with extended hemodynamic monitoring, analyzing process-of-care variables for the first week of ICU admission. The primary outcome parameter was 28-day mortality. ΔmaxEVLWI indicated the maximum difference between EVLWI measurements during ICU stay. Patients with a ΔmaxEVLWI <-2 mL/kg were called 'responders'. CLI was defined as C-reactive protein (milligrams per deciliter) over albumin (grams per liter) ratio and conservative late fluid management (CLFM) as even-to-negative fluid balance on at least two consecutive days.
Results: CLI had a biphasic course. ΔmaxEVLWI was lower if CLFM was achieved and in survivors (-2.4 ± 4.8 vs 1.0 ± 5.5 mL/kg, p = 0.001; -3.3 ± 3.8 vs 2.5 ± 5.3 mL/kg, p = 0.001, respectively). No CLFM achievement was associated with increased CLI and IAPmean on day 3 and higher risk to be nonresponder (odds ratio (OR) 2.76, p = 0.046; OR 1.28, p = 0.011; OR 5.52, p = 0.001, respectively). Responders had more ventilator-free days during the first week (2.5 ± 2.3 vs 1.5 ± 2.3, p = 0.023). Not achieving CLFM and being nonresponder were strong independent predictors of mortality (OR 9.34, p = 0.001 and OR 7.14, p = 0.001, respectively).
Conclusion: There seems to be an important correlation between CLI, EVLWI kinetics, IAP, and fluid balance in mechanically ventilated patients, associated with organ dysfunction and poor prognosis. In this context, we introduce the global increased permeability syndrome.
Keywords: abdominal pressure; capillary leak; extravascular lung water; fluid balance; fluid management; organ failure; prognosis.
Figures




References
-
- Bone RC. Immunologic dissonance: a continuing evolution in our understanding of the systemic inflammatory response syndrome (SIRS) and the multiple organ dysfunction syndrome (MODS) Annals of internal medicine. 1996;125(8):680–687. - PubMed
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M. Early goal-directed therapy in the treatment of severe sepsis and septic shock. The New England journal of medicine. 2001;345(19):1368–1377. - PubMed
-
- Guyton AC. Interstitial fluid pressure. II. Pressure-volume curves of interstitial space. Circulation research. 1965;16:452–460. - PubMed
-
- Staub NC. The pathogenesis of pulmonary edema. Progress in cardiovascular diseases. 1980;23(1):53–80. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
