

Moderate intra-abdominal hypertension is associated with an increased lactate-pyruvate ratio in the rectus abdominis muscle tissue: a pilot study during laparoscopic surgery
- PMID: 22873415
- PMCID: PMC3390303
- DOI: 10.1186/2110-5820-2-S1-S14
Moderate intra-abdominal hypertension is associated with an increased lactate-pyruvate ratio in the rectus abdominis muscle tissue: a pilot study during laparoscopic surgery
Abstract
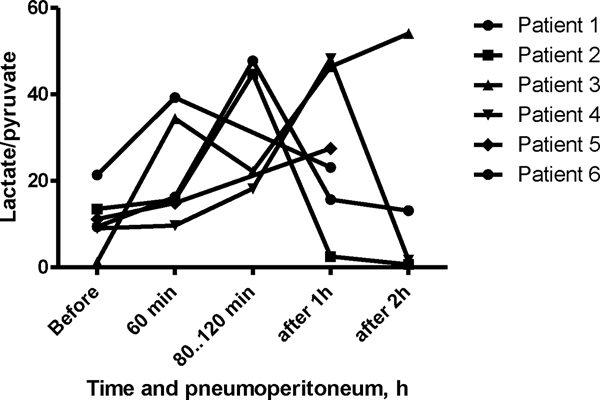
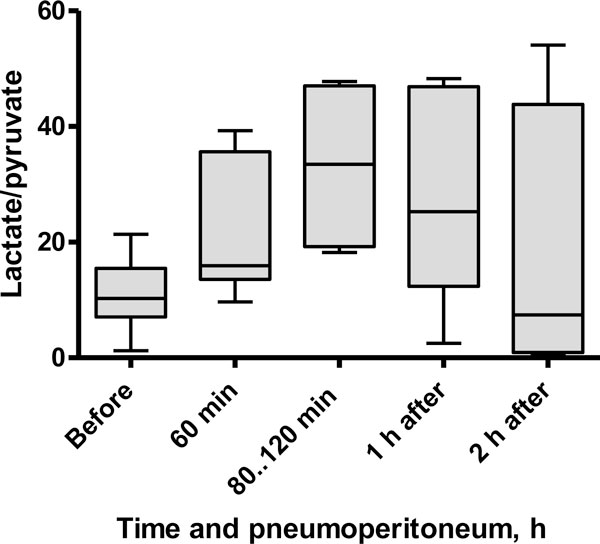
Background: The development of intra-abdominal hypertension [IAH] in critically ill patients admitted to the ICU is an independent predictor of mortality. In an attempt to find an early, clinically relevant metabolic signal of modest IAH, we investigated abdominal wall metabolite concentrations in a small group of patients undergoing laparoscopic surgery. We hypothesized that elevated intra-abdominal pressure [IAP] due to pneumoperitoneum leads to an increased lactate/pyruvate [L/P] ratio in the rectus abdominis muscle [RAM], indicating anaerobic metabolism.
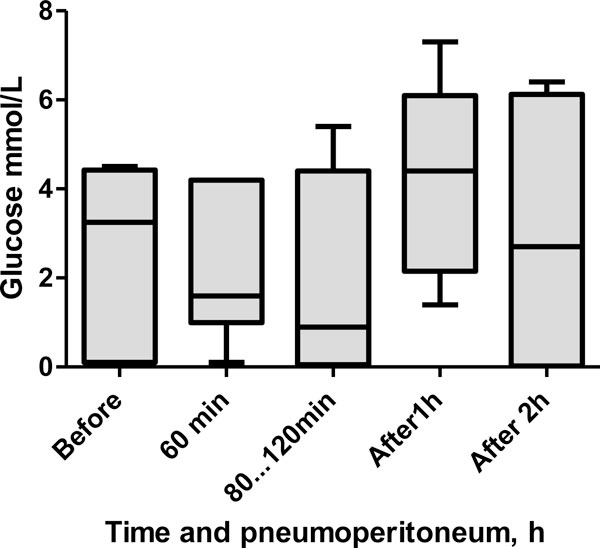
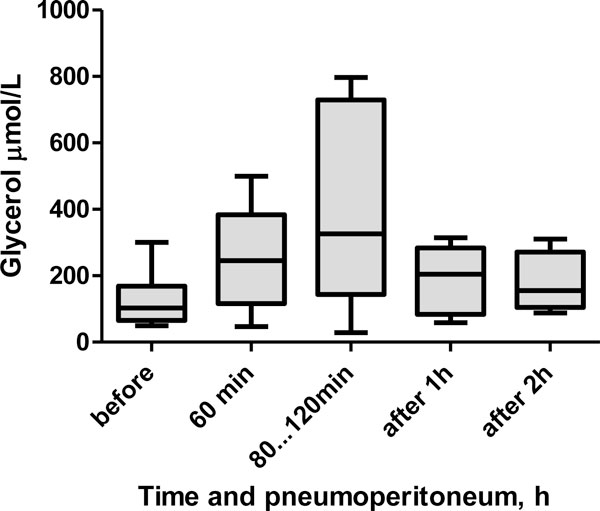
Method: Six patients scheduled for elective laparoscopic gastric fundoplication were studied. Two hours before surgery, a microdialysis catheter (CMA 60, CMA Small Systems AB, Solna, Sweden) was inserted into the RAM under local anaesthesia. Catheter placement was confirmed by ultrasound. The microdialysis perfusion rate was set at 0.3 μL/min. Dialysate was collected hourly prior to pneumoperitoneum, during pneumoperitoneum, and for 2 h after pneumoperitoneum resolution. IAP was maintained at 12 to 13 mmHg during the surgery. The glucose, glycerol, pyruvate and lactate contents of the dialysate were measured.
Results: The median (interquartile range) L/P ratio was 10.3 (7.1 to 15.5) mmol/L at baseline. One hour of pneumoperitoneum increased the L/P ratio to 16.0 (13.6 to 35.3) mmol/L (p = 0.03). The median pneumoperitoneum duration was 86 (77 to 111) min. The L/P ratio at 2 h post-pneumoperitoneum was not different from that at baseline (p = 1.0). No changes in glycerol or glucose levels were observed.
Conclusions: IAH of 12 to 13 mmHg, even for a relatively short duration, is associated with metabolic changes in the abdominal wall muscle tissue of patients undergoing laparoscopic surgery. We suggest that tissue hypoperfusion occurs even during a modest increase in IAP, and intramuscular metabolic monitoring could therefore serve as an early warning sign of deteriorating tissue perfusion.
Figures
Similar articles
-
Moderate intra-abdominal hypertension leads to anaerobic metabolism in the rectus abdominis muscle tissue of critically ill patients: a prospective observational study.Biomed Res Int. 2014;2014:857492. doi: 10.1155/2014/857492. Epub 2014 Mar 13. Biomed Res Int. 2014. PMID: 24745026 Free PMC article. Clinical Trial.
-
Early detection of subclinical organ dysfunction by microdialysis of the rectus abdominis muscle in a porcine model of critical intra-abdominal hypertension.Shock. 2012 Oct;38(4):420-8. doi: 10.1097/SHK.0b013e31825ef7e7. Shock. 2012. PMID: 22683730
-
Microdialysis of the rectus abdominis muscle for early detection of impending abdominal compartment syndrome.Intensive Care Med. 2007 Aug;33(8):1434-43. doi: 10.1007/s00134-007-0725-9. Epub 2007 Jun 19. Intensive Care Med. 2007. PMID: 17576536
-
[The patient with intra-abdominal hypertension].Anasthesiol Intensivmed Notfallmed Schmerzther. 2016 Jan;51(1):8-16. doi: 10.1055/s-0041-103160. Epub 2016 Feb 10. Anasthesiol Intensivmed Notfallmed Schmerzther. 2016. PMID: 26863642 Review. German.
-
What's new in medical management strategies for raised intra-abdominal pressure: evacuating intra-abdominal contents, improving abdominal wall compliance, pharmacotherapy, and continuous negative extra-abdominal pressure.Anaesthesiol Intensive Ther. 2015;47(1):54-62. doi: 10.5603/AIT.a2014.0065. Epub 2014 Nov 25. Anaesthesiol Intensive Ther. 2015. PMID: 25421926 Review.
Cited by
-
Essential hypertension: A filtered serum based metabolomics study.Sci Rep. 2017 May 19;7(1):2153. doi: 10.1038/s41598-017-02289-9. Sci Rep. 2017. PMID: 28526818 Free PMC article.
-
A multifaceted individualized pneumoperitoneum strategy for laparoscopic colorectal surgery: a multicenter observational feasibility study.Surg Endosc. 2019 Jan;33(1):252-260. doi: 10.1007/s00464-018-6305-y. Epub 2018 Jun 27. Surg Endosc. 2019. PMID: 29951750
-
Moderate intra-abdominal hypertension leads to anaerobic metabolism in the rectus abdominis muscle tissue of critically ill patients: a prospective observational study.Biomed Res Int. 2014;2014:857492. doi: 10.1155/2014/857492. Epub 2014 Mar 13. Biomed Res Int. 2014. PMID: 24745026 Free PMC article. Clinical Trial.
-
An individualised versus a conventional pneumoperitoneum pressure strategy during colorectal laparoscopic surgery: rationale and study protocol for a multicentre randomised clinical study.Trials. 2019 Apr 3;20(1):190. doi: 10.1186/s13063-019-3255-1. Trials. 2019. PMID: 30944044 Free PMC article.
-
Low intra-abdominal pressure and deep neuromuscular blockade laparoscopic surgery and surgical space conditions: A meta-analysis.Medicine (Baltimore). 2020 Feb;99(9):e19323. doi: 10.1097/MD.0000000000019323. Medicine (Baltimore). 2020. PMID: 32118762 Free PMC article.
References
-
- Malbrain ML, Chiumello D, Pelosi P, Bihari D, Innes R, Ranieri VM, Del Turco M, Wilmer A, Brienza N, Malcangi V, Cohen J, Japiassu A, De Keulenaer BL, Daelemans R, Jacquet L, Laterre PF, Frank G, de Souza P, Cesana B, Gattinoni L. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multiple-center epidemiological study. Crit Care Med. 2005;33:315–322. doi: 10.1097/01.CCM.0000153408.09806.1B. - DOI - PubMed
-
- Malbrain ML, Cheatham ML, Kirkpatrick A, Sugrue M, Parr M, De Waele J, Balogh Z, Leppäniemi A, Olvera C, Ivatury R, D'Amours S, Wendon J, Hillman K, Johansson K, Kolkman K, Wilmer A. Results from the International Conference of Experts on Intra-abdominal Hypertension and Abdominal Compartment Syndrome. I. Definitions. Intensive Care Med. 2006;32:1722–1732. doi: 10.1007/s00134-006-0349-5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
