

Aiming for a negative fluid balance in patients with acute lung injury and increased intra-abdominal pressure: a pilot study looking at the effects of PAL-treatment
- PMID: 22873416
- PMCID: PMC3390296
- DOI: 10.1186/2110-5820-2-S1-S15
Aiming for a negative fluid balance in patients with acute lung injury and increased intra-abdominal pressure: a pilot study looking at the effects of PAL-treatment
Abstract
Introduction: Achievement of a negative fluid balance in patients with capillary leak is associated with improved outcome. We investigated the effects of a multi-modal restrictive fluid strategy aiming for negative fluid balance in patients with acute lung injury (ALI).
Methods: In this retrospective matched case-control study, we included 114 mechanically ventilated (MV) patients with ALI. We compared outcomes between a group of 57 patients receiving PAL-treatment (PAL group) and a matched control group, abstracted from a historical cohort. PAL-treatment combines high levels of positive end-expiratory pressure, small volume resuscitation with hyperoncotic albumin, and fluid removal with furosemide (Lasix®) or ultrafiltration. Effects on extravascular lung water index (EVLWI), intra-abdominal pressure (IAP), organ function, and vasopressor therapy were recorded during 1 week. The primary outcome parameter was 28-day mortality.
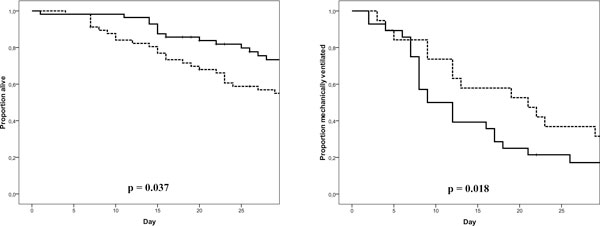
Results: At baseline, no significant intergroup differences were found, except for lower PaO2/FIO2 and increased IAP in the PAL group (174.5 ± 84.5 vs 256.5 ± 152.7, p = 0.001; 10.0 ± 4.2 vs 8.0 ± 3.7 mmHg, p = 0.013, respectively). After 1 week, PAL-treated patients had a greater reduction of EVLWI, IAP, and cumulative fluid balance (-4.2 ± 5.6 vs -1.1 ± 3.7 mL/kg, p = 0.006; -0.4 ± 3.6 vs 1.8 ± 3.8 mmHg, p = 0.007; -1,451 ± 7,761 vs 8,027 ± 5,254 mL, p < 0.001). Repercussions on cardiovascular and renal function were limited. PAL-treated patients required fewer days of intensive care unit admission and days on MV (23.6 ± 15 vs 37.1 ± 19.9 days, p = 0.006; 14.6 ± 10.7 vs 25.5 ± 20.2 days, respectively) and had a lower 28-day mortality (28.1% vs 49.1%, p = 0.034).
Conclusion: PAL-treatment in patients with ALI is associated with a negative fluid balance, a reduction of EVLWI and IAP, and improved clinical outcomes without compromising organ function.
Figures



References
-
- Prowle JR, Echeverri JE, Ligabo EV, Ronco C, Bellomo R. Fluid balance and acute kidney injury. Nature reviews. 2010;6(2):107–115. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
