

Recognition and management of abdominal compartment syndrome among German pediatric intensivists: results of a national survey
- PMID: 22873424
- PMCID: PMC3390295
- DOI: 10.1186/2110-5820-2-S1-S8
Recognition and management of abdominal compartment syndrome among German pediatric intensivists: results of a national survey
Abstract
Introduction: Several decades ago, the beneficial effects of goal-directed therapy, which include decompressive laparotomy (DL) and open abdomen procedures in cases of intra-abdominal hypertension (IAH) in children, were proven in the context of closures of abdominal wall defects and large-for-size organ transplantations. Different neonatologic and pediatric disease patterns are also known to be capable of increasing intra-abdominal pressure (IAP). Nevertheless, a considerable knowledge transfer regarding such risk factors has hardly taken place. When left undetected and untreated, IAH threatens to evolve into abdominal compartment syndrome (ACS), which is accompanied by a mortality rate of up to 60% in children. Therefore, the present study looks at the recognition and knowledge of IAH/ACS among German pediatric intensivists.
Methods: In June 2010, a questionnaire was mailed to the heads of pediatric intensive care units of 205 German pediatric hospitals.
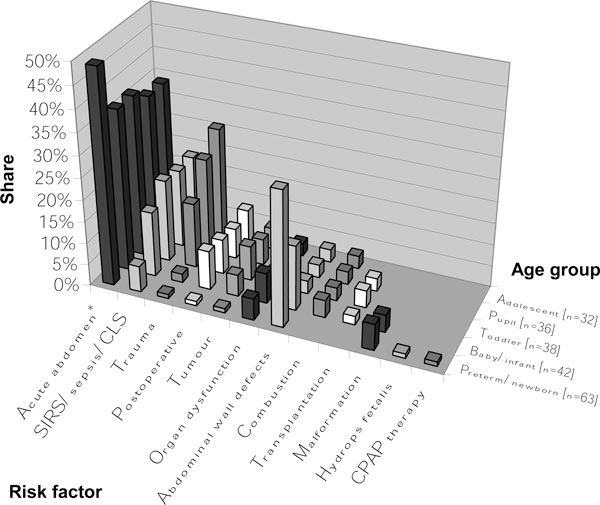
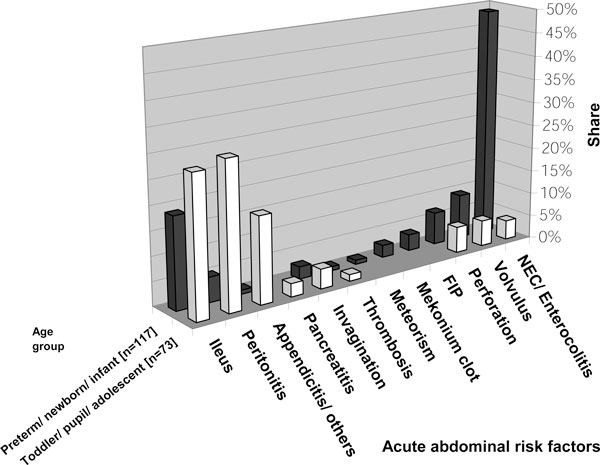
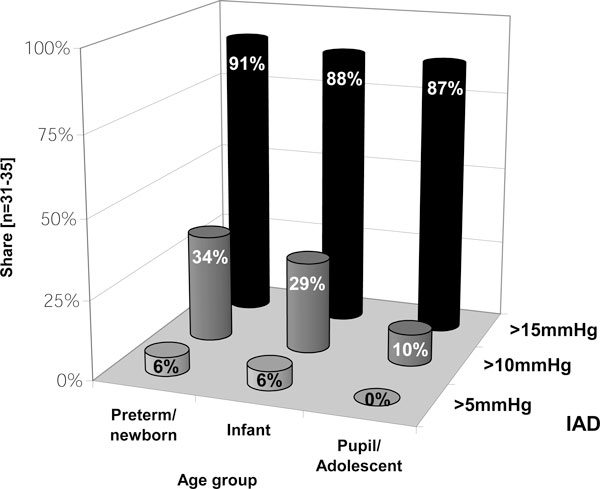
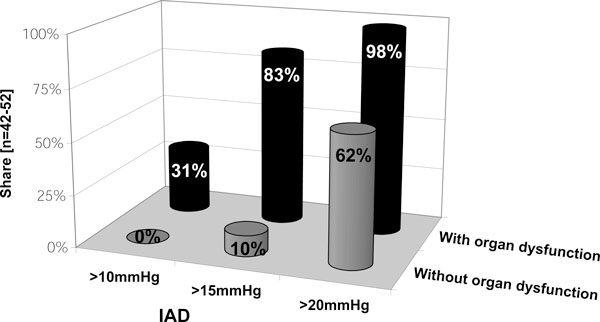
Results: The response rate was 62%. At least one case of IAH was reported by 36% of respondents; at least one case of ACS, by 25%. Compared with adolescents, younger critically ill children appeared to develop IAH/ACS more often. Routine measurements of IAP were said to be performed by 20% of respondents. Bladder pressure was used most frequently (96%) to assess IAP. Some respondents (17%) only measured IAP in cases of organ dysfunction and failure. In 2009, the year preceding this study, 21% of respondents claimed to have performed a DL. Surgical decompression was indicated if signs of organ dysfunction were present. This was also done in cases of at least grade III IAH (IAP > 15 mmHg) without organ impairment.
Conclusions: Although awareness among pediatricians appears to have been increasing over the last decade, definitions and guidelines regarding the diagnosis and management of IAH/ACS are not applied uniformly. This variability could express an ever present lack of awareness and solid prospective data.
Figures
References
-
- Gross RE. A new method for surgical treatment of large omphaloceles. Surgery. 1948;24:277–292. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
