

Endoscopic stenting for hilar cholangiocarcinoma: efficacy of unilateral and bilateral placement of plastic and metal stents in a retrospective review of 480 patients
- PMID: 22873816
- PMCID: PMC3476445
- DOI: 10.1186/1471-230X-12-103
Endoscopic stenting for hilar cholangiocarcinoma: efficacy of unilateral and bilateral placement of plastic and metal stents in a retrospective review of 480 patients
Abstract
Background: Endoscopic biliary drainage of hilar cholangiocarcinoma is controversial with respect to the optimal types of stents and the extent of drainage. This study evaluated endoscopic palliation in patients with hilar cholangiocarcinoma using self-expandable metallic stents (SEMS) and plastic stents (PS).We also compared unilateral and bilateral stent placement according to the Bismuth classification.
Methods: Data on 480 patients receiving endoscopic biliary drainage for hilar cholangiocarcinoma between September 1995 and December 2010 were retrospectively reviewed to evaluate the following outcome parameters: technical success (TS), functional success (FS), early and late complications, stent patency and survival. Patients were followed from stent insertion until death or stent occlusion. Patients were divided into 3 groups according to the Bismuth classification (Group 1, type I; Group 2, type II; Group 3, type ≥ III).
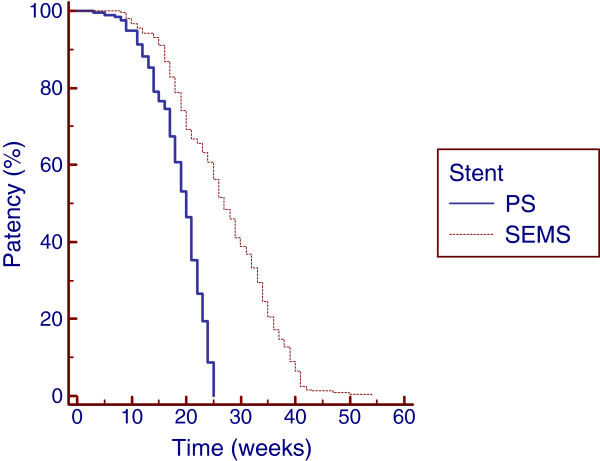
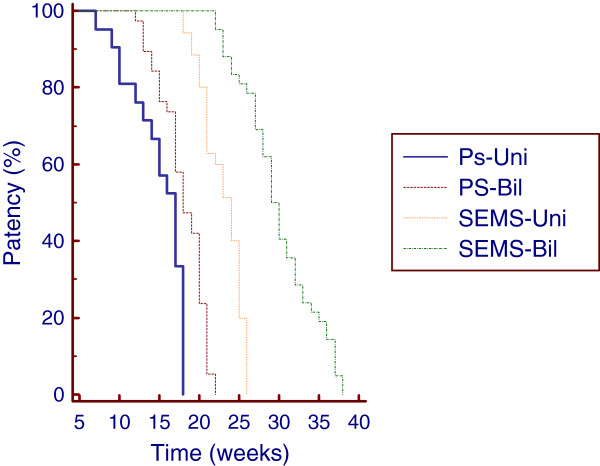
Results: The initial stent insertion was successful in 450 (93.8%) patients. TS was achieved in 204 (88.3%) patients treated with PS and in 246 (98.8%) patients palliated with SEMS (p < 0.001). In the intention-to-treat (ITT) analysis, the FS in patients treated with SEMS (97.9%) was significantly higher than in patients treated with PS (84.8%) (p < 0.001). Late complications occurred in 115 (56.4%) patients treated with PS and 60 (24.4%) patients treated with SEMS (p < 0.001). The median duration of stent patency in weeks (w) were as follows: 20 w in patients palliated with PS and 27 w in patients treated with SEMS (p < 0.0001). In Group 2, the median duration of PS patency was 17 w and 18 w for unilateral and bilateral placement, respectively (p = 0.0004); the median duration of SEMS patency was 24 w and 29 w for unilateral and bilateral placement, respectively (p < 0.0001). Multivariate analysis using the Poisson regression showed that SEMS placement (B = 0.48; P < 0.01) and bilateral deployment (B = 0.24; P < 0.01) were the only independent prognostic factors associated with stent patency.
Conclusions: SEMS insertion for the palliation of hilar cholangiocarcinoma offers higher technical and clinical success rates in the ITT analysis as well as lower complication rates and a superior cumulative stent patency when compared with PS placement in all Bismuth classifications. The cumulative patency of bilateral SEMS or PS stents was significantly higher than that of unilateral SEMS or PS stents, with lower occlusion rates in Bismuth II patients.
Figures
Similar articles
-
Optimum palliation of inoperable hilar cholangiocarcinoma: comparative assessment of the efficacy of plastic and self-expanding metal stents.Dig Dis Sci. 2011 May;56(5):1557-64. doi: 10.1007/s10620-010-1550-5. Epub 2011 Jan 11. Dig Dis Sci. 2011. PMID: 21222156
-
Palliative treatment with self-expandable metallic stents in patients with advanced type III or IV hilar cholangiocarcinoma: a percutaneous versus endoscopic approach.Gastrointest Endosc. 2009 Jan;69(1):55-62. doi: 10.1016/j.gie.2008.04.005. Epub 2008 Jul 26. Gastrointest Endosc. 2009. PMID: 18657806
-
Y-shaped endoscopic bilateral metal stent placement for malignant hilar biliary obstruction: prospective long-term study.Scand J Gastroenterol. 2011 Mar;46(3):326-32. doi: 10.3109/00365521.2010.536253. Epub 2010 Nov 17. Scand J Gastroenterol. 2011. PMID: 21082874 Clinical Trial.
-
Endoscopic drainage in patients with inoperable hilar cholangiocarcinoma.Korean J Intern Med. 2013 Jan;28(1):8-18. doi: 10.3904/kjim.2013.28.1.8. Epub 2012 Dec 28. Korean J Intern Med. 2013. PMID: 23345990 Free PMC article. Review.
-
Technical tips and issues of biliary stenting, focusing on malignant hilar obstruction.Minerva Gastroenterol Dietol. 2014 Jun;60(2):135-49. Minerva Gastroenterol Dietol. 2014. PMID: 24780948 Review.
Cited by
-
Association between progression-free survival and metal stent patency in patients with advanced pancreatic cancer.J Gastrointest Oncol. 2022 Aug;13(4):1981-1988. doi: 10.21037/jgo-22-218. J Gastrointest Oncol. 2022. PMID: 36092328 Free PMC article.
-
Update on Pancreatobiliary Stents: Stent Placement in Advanced Hilar Tumors.Clin Endosc. 2015 May;48(3):201-8. doi: 10.5946/ce.2015.48.3.201. Epub 2015 May 29. Clin Endosc. 2015. PMID: 26064819 Free PMC article. Review.
-
Unilateral multiple metallic stent-in-stent for a case of hilar biliary cancer: an alternative stenting strategy.Saudi J Gastroenterol. 2014 May-Jun;20(3):199-201. doi: 10.4103/1319-3767.133035. Saudi J Gastroenterol. 2014. PMID: 24976285 Free PMC article.
-
Endoscopic palliation of malignant biliary strictures.World J Gastrointest Oncol. 2016 Mar 15;8(3):240-7. doi: 10.4251/wjgo.v8.i3.240. World J Gastrointest Oncol. 2016. PMID: 26989459 Free PMC article. Review.
-
Ampullary Metastasis From Breast Cancer: A Rare Cause of Obstructive Jaundice.GE Port J Gastroenterol. 2016 Jun 21;23(6):300-303. doi: 10.1016/j.jpge.2016.03.001. eCollection 2016 Nov-Dec. GE Port J Gastroenterol. 2016. PMID: 28868483 Free PMC article.
References
-
- Cheng JL, Bruno MJ, Bergman JJ, Rauws EA, Tytgat GN, Huibregtse K. Endoscopic palliation of patients with biliary obstruction caused by nonresectable hilar cholangiocarcinoma: efficacy of self-expandable metallic Wallstents. Gastrointest Endosc. 2005;56:33–39. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
