

Disordered follicle development
- PMID: 22874072
- PMCID: PMC3727408
- DOI: 10.1016/j.mce.2012.07.011
Disordered follicle development
Abstract
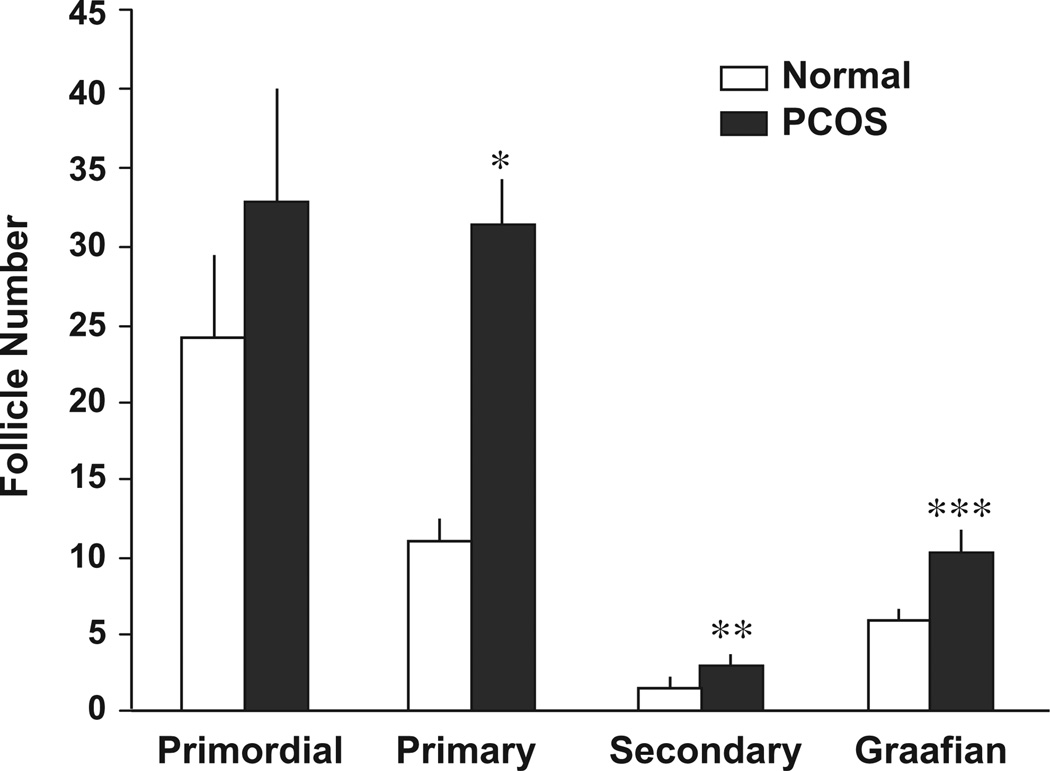
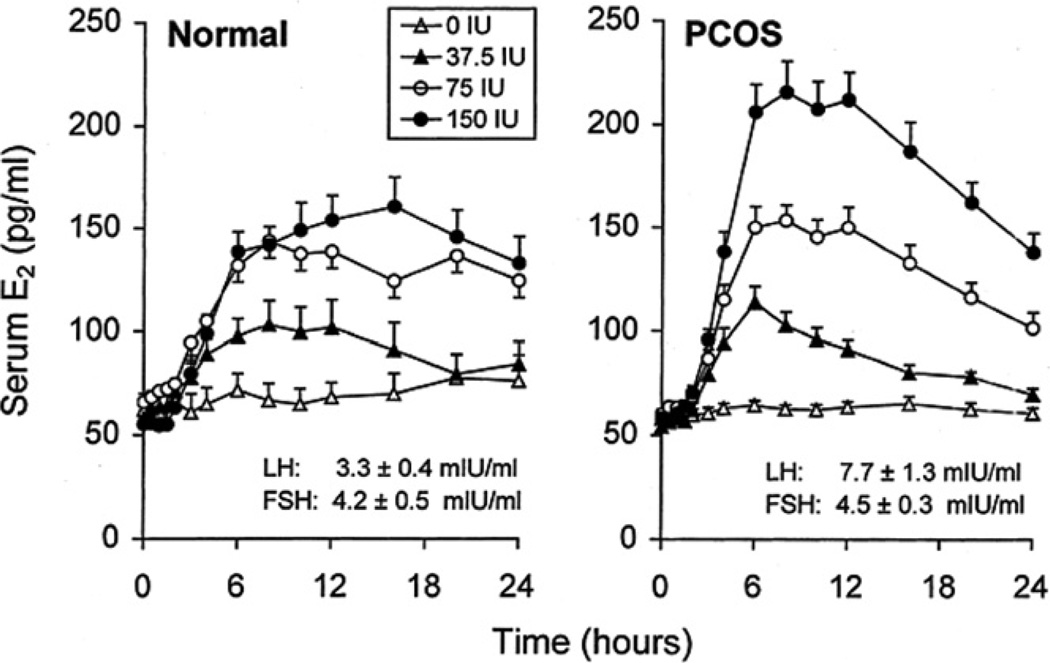
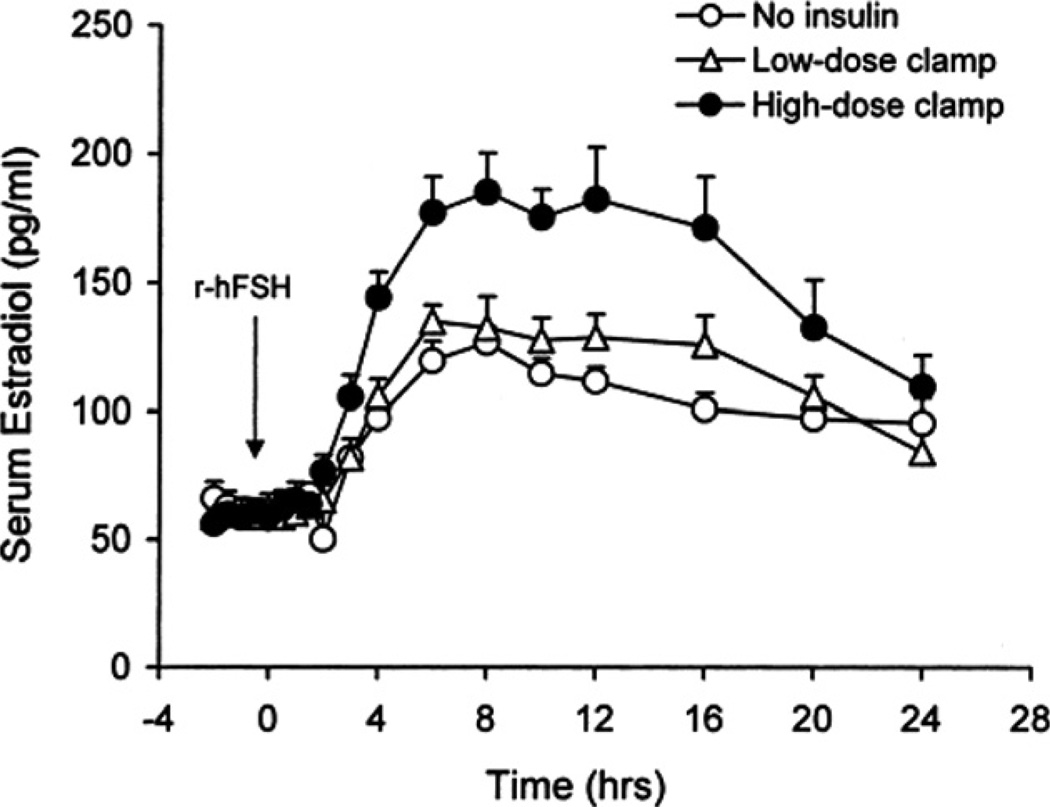
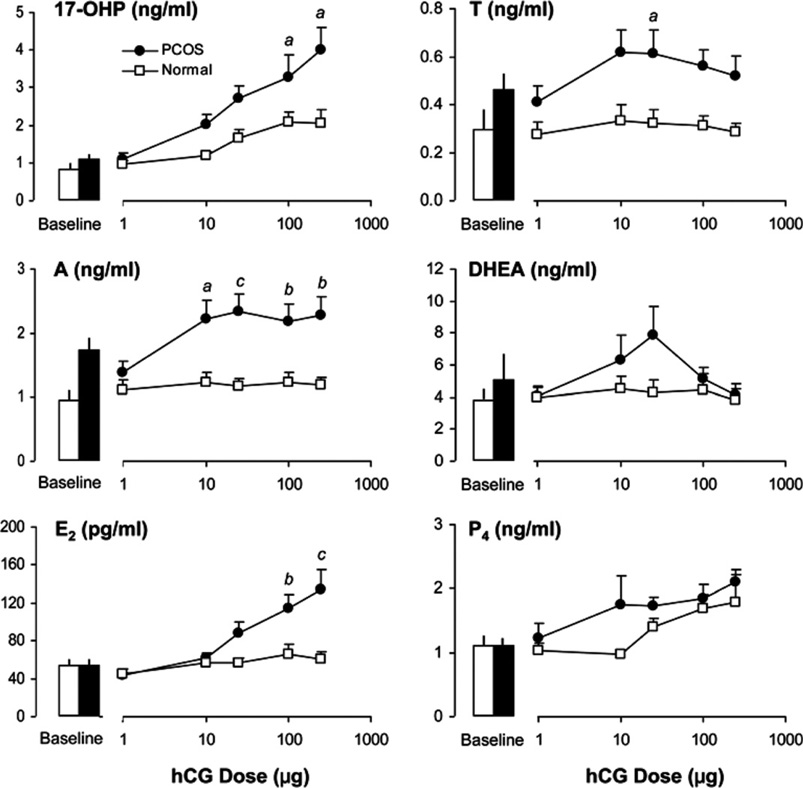
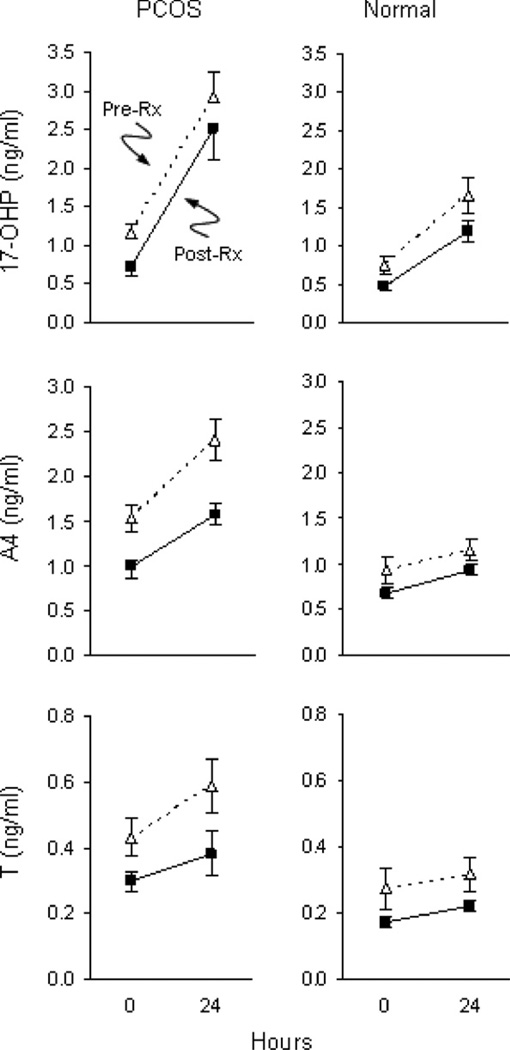
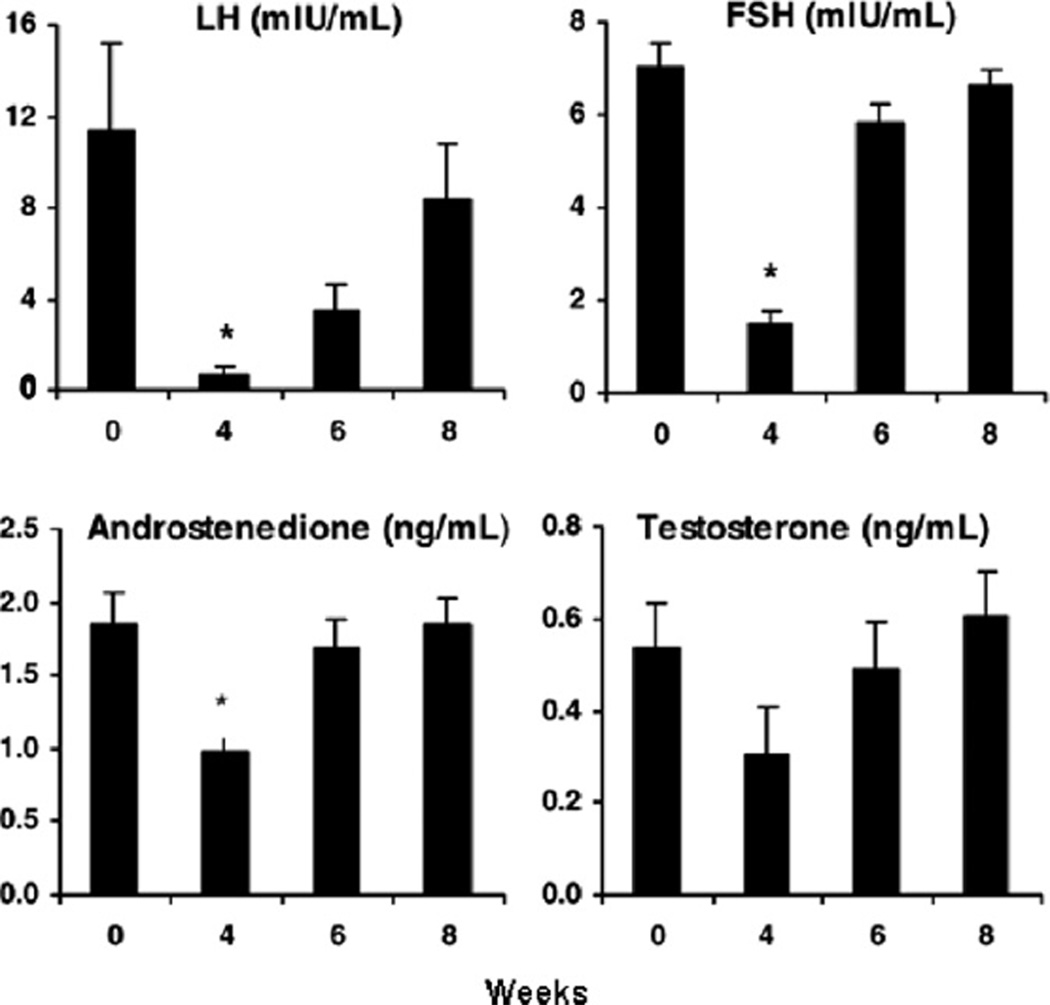
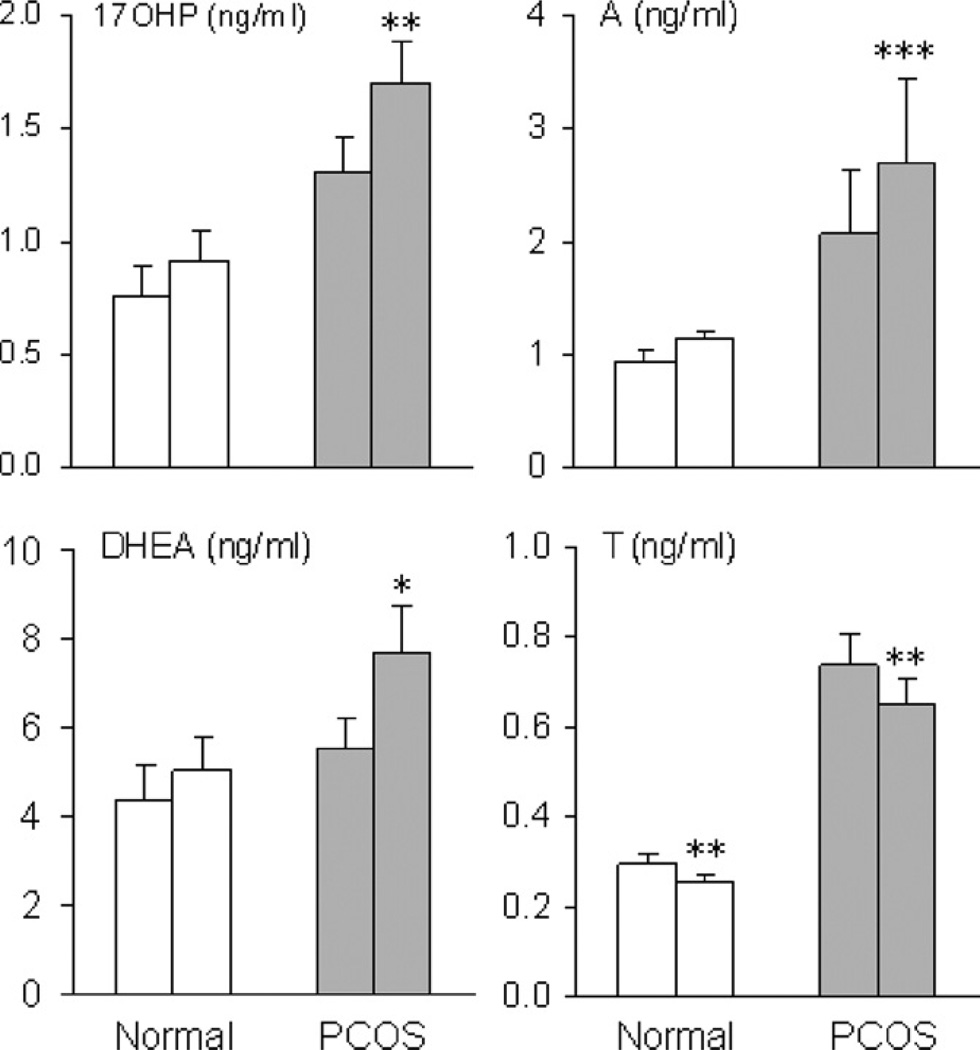
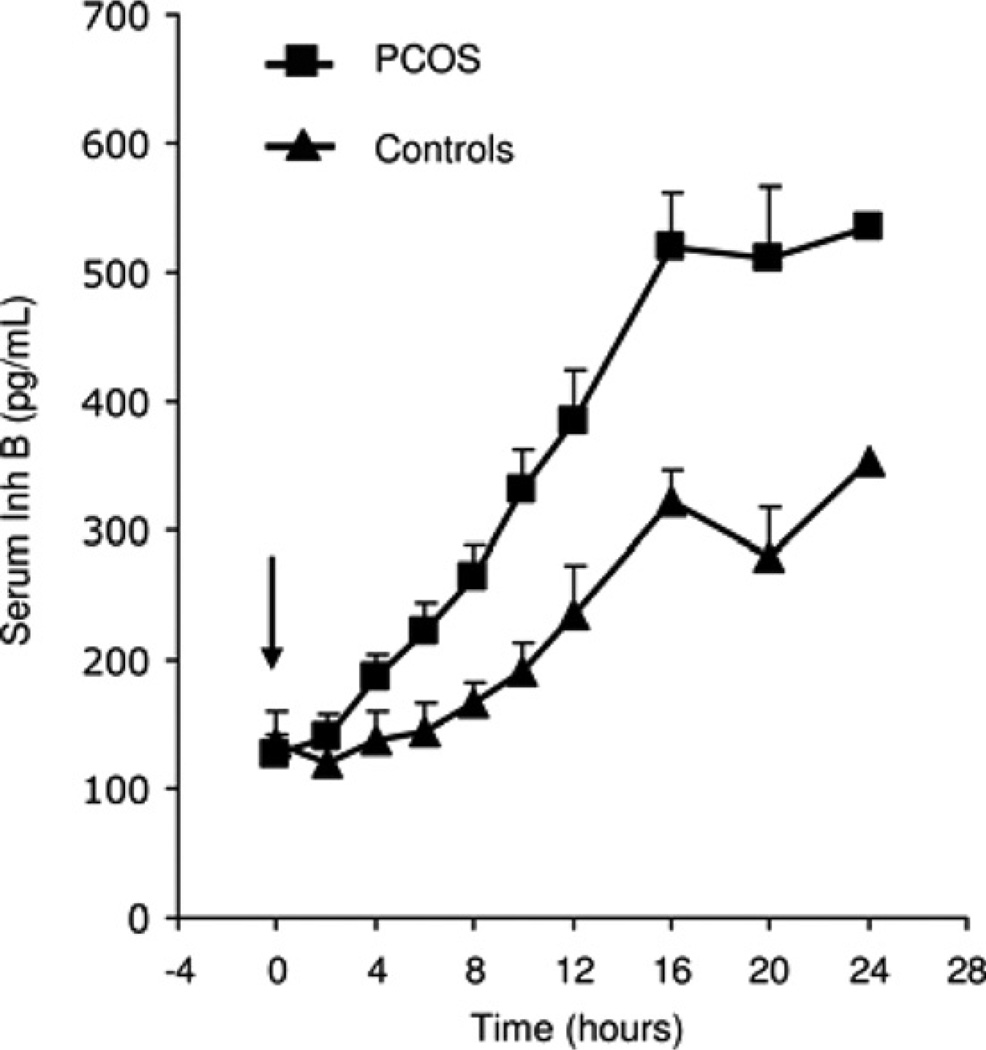
Alterations of ovarian follicle morphology and function have been well documented in women with PCOS. These include increased numbers of growing preantral follicles, failure of follicle growth beyond the mid-antral stage, evidence of granulosa call degeneration, and theca cell hyperplasia. Functional abnormalities include paradoxical granulosa cell hyperresponsiveness to FSH which is clinically linked to ovarian hyperstimulation during ovulation induction. In addition, there is likely a primary theca cell defect that accounts for the majority of excess androgen production in this disorder. The precise mechanisms responsible for altered follicle function are not completely clear. However, several factors appear to influence normal advancement of follicle development as well as impair ovarian steroidogenesis. These include intra- as well as extraovarian influences that distort normal ovarian growth and disrupt steroid production by follicle cells.
Published by Elsevier Ireland Ltd.
Figures
References
-
- Adashi EY, Hsueh AJW. Estrogens augment the stimulation of ovarian aromatase activity by follicle-stimulating hormone in cultured rat granulose cells. J. Biol. Chem. 1982;257:6077–6083. - PubMed
-
- Almahbobi G, Anderiesz C, Hutchinson P, McFarlane JR, Wood C, Trounson AO. Functional integrity of granulosa cells from polycystic ovaries. Clin. Endocrinol. 1996;44:571–580. - PubMed
-
- Barbieri RL, Makris A, Ryan KJ. Insulin stimulates androgen accumulation in incubations of human ovarian stroma and theca. Obstet. Gynecol. 1984;64:73S–80S. - PubMed
-
- Barbieri RL, Makris A, Randall RW, Daniels G, Kistner RW, Ryan KJ. Insulin stimulates androgen accumulation in incubations of ovarian stroma obtained from women with hyperandrogenism. J. Clin. Endocrinol. Metab. 1986;62:904–910. - PubMed
-
- Barnes RB, Rosenfield RL, Burstein S, Ehrmann DA. Pituitary-ovarian responses to nafarelin testing in the polycystic ovary syndrome. N. Engl. J. Med. 1989;320:559–565. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
