

Colorectal cancer in inflammatory bowel disease: what is the real magnitude of the risk?
- PMID: 22876036
- PMCID: PMC3413056
- DOI: 10.3748/wjg.v18.i29.3839
Colorectal cancer in inflammatory bowel disease: what is the real magnitude of the risk?
Abstract
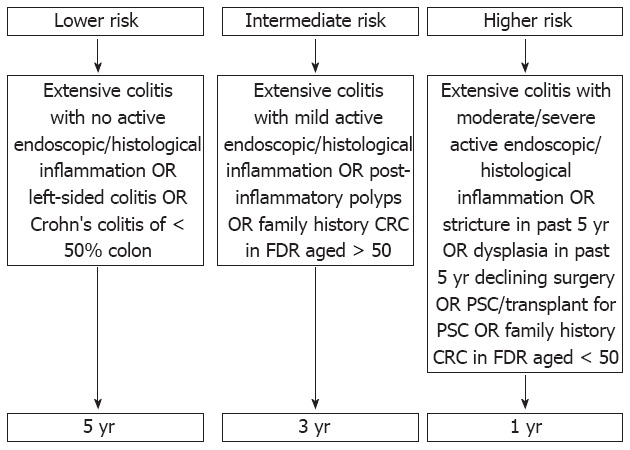
The association between inflammatory bowel disease (IBD) and colorectal cancer (CRC) has been recognised since 1925 and still accounts for 10%-15% of deaths in IBD. IBD-associated CRC (IBD-CRC) affects patients at a younger age than sporadic CRC. The prognosis for sporadic CRC and IBD-CRC is similar, with a 5-year survival of approximately 50%. Identifying at risk patients and implementing appropriate surveillance for these patients is central to managing the CRC risk in IBD. The increased risk of colorectal cancer in association with IBD is thought to be due to genetic and acquired factors. The link between inflammation and cancer is well recognised but the molecular biology, immune pathobiology and genetics of IBD-CRC are areas of much ongoing research. This review examines the literature relating to IBD-CRC, focusing on the incidence of IBD-CRC and examining potential risk factors including age at diagnosis, gender, duration and extent of colitis, severity of inflammation, family history of sporadic CRC and co-existent primary sclerosing cholangitis (PSC). Confirmed risk factors for IBD-CRC are duration, severity and extent of colitis, the presence of co-existent PSC and a family history of CRC. There is insufficient evidence currently to support an increased frequency of surveillance for patients diagnosed with IBD at a younger age. Evidence-based guidelines advise surveillance colonoscopy for patients with colitis 8 to 10 years after diagnosis, with the interval for further surveillance guided by risk factors (extent of disease, family history of CRC, post-inflammatory polyps, concomitant PSC, personal history of colonic dysplasia, colonic strictures). There is a move away from using random colonic biopsies towards targeted biopsies aimed at abnormal areas identified by newer colonoscopic techniques (narrow band imaging, chromoendoscopy, confocal microendoscopy).
Keywords: Colorectal cancer; Crohn’s disease; Inflammatory bowel disease; Risk; Ulcerative colitis.
Figures
References
-
- Crohn BB. The sigmoidoscopic picture of chronic ulcerative colitis (non-specific) Amer J Med Sci. 1925;170:220–228.
-
- Munkholm P. Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease. Aliment Pharmacol Ther. 2003;18 Suppl 2:1–5. - PubMed
-
- Calkins BM, Lilienfeld AM, Garland CF, Mendeloff AI. Trends in incidence rates of ulcerative colitis and Crohn’s disease. Dig Dis Sci. 1984;29:913–920. - PubMed
-
- Munkholm P, Loftus EV, Reinacher-Schick A, Kornbluth A, Mittmann U, Esendal B. Prevention of colorectal cancer in inflammatory bowel disease: value of screening and 5-aminosalicylates. Digestion. 2006;73:11–19. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
