

A totally mini-invasive approach for colorectal laparoscopic surgery
- PMID: 22876039
- PMCID: PMC3413059
- DOI: 10.3748/wjg.v18.i29.3869
A totally mini-invasive approach for colorectal laparoscopic surgery
Abstract
Aim: To study the short-term outcome of patients treated with laparoscopic right colectomy and how intracorporeal anastomosis has improved the outcome.
Methods: We retrospectively examined all patients affected by colorectal cancer who underwent a laparoscopic right colectomy between January 2006 and December 2010 in our department. Our evaluation criteria were: diagnosis of colorectal carcinoma at presurgical biopsy, elective surgery, and the same surgeon. We excluded: emergency surgery, conversions from laparotomic colectomy, and other surgeons. The endpoints we examined were: surgical time, number of lymph nodes removed, length of stay (removal of nasogastric tube, bowel movements, gas evacuation, solid and liquid feeding, hospitalization), and major complications. Seventy-two patients were divided into two groups: intracorporeal anastomosis (39 patients) and extracorporeal anastomosis (33 patients).
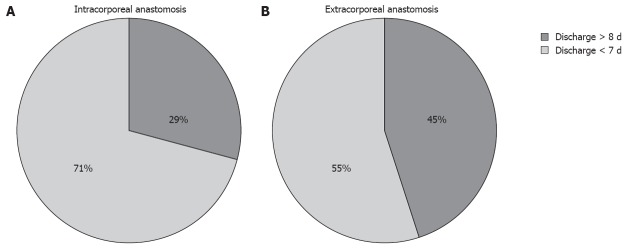
Results: Significant differences were observed between intracorporeal vs extracorporeal anastomosis, respectively, for surgical times (186.8 min vs 184.1 min, P < 0.001), time to resumption of gas evacuation (3 d vs 3.5 d, P < 0.001), days until resumption of bowel movements (3.8 d vs 4.9 d, P < 0.001), days until resumption of liquid diet (3.5 d vs 4.5 d, P < 0.001), days until resuming a solid diet (4.6 d vs 5.7 d, P < 0.001), and total hospitalization duration (7.4 d vs 8.5 d, P < 0.001). In the intracorporeal group, on average, 19 positive lymph nodes were removed; in the extracorporeal group, on average, 14 were removed P < 0.001). Thus, intracorporeal anastomosis for right laparoscopic colectomy improved patient outcome by providing faster recovery of nutrition, faster recovery of intestinal function, and shorter hospitalization than extracorporeal anastomosis.
Conclusion: Short-term outcomes favor intracorporeal anastomosis, confirming that a less traumatic surgical approach improves patient outcome.
Keywords: Anastomosis; Cancer; Colorectal disease; Laparoscopy; Surgery.
Figures
References
-
- Tinmouth J, Tomlinson G. Laparoscopically assisted versus open colectomy for colon cancer. N Engl J Med. 2004;351:933–934. - PubMed
-
- Guillou PJ, Quirke P, Thorpe H, Walker J, Jaine DG, Smith AMH, Heath RM, Brown JM. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre randomized controlled trail. Lancet. 2005;365:1718–1726. - PubMed
-
- Lacy AM, Garcia-Valdecasas JC, Pique JM, Delgado S, Campo E, Bordas JM, Taurá P, Grande L, Fuster J, Pacheco JL. Short-term outcome analysis of a randomized study comparing laparoscopic vs open colectomy for colon cancer. Surg Endosc. 1995;9:1101–1105. - PubMed
-
- COLOR Study Group. COLOR: a randomized clinical trial comparing laparoscopic and open resection for colon cancer. Dig Surg. 2000;17:617–622. - PubMed
-
- Fabozzi M, Allieta R, Contul RB, Grivon M, Millo P, Lale-Murix E, Nardi M. Comparison of short- and medium-term results between laparoscopically assisted and totally laparoscopic right hemicolectomy: a case-control study. Surg Endosc. 2010;24:2085–2091. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
